- Tổng quan
- Nội dung
- VB gốc
- Tiếng Anh
- Hiệu lực
- VB liên quan
- Lược đồ
-
Nội dung hợp nhất
Tính năng này chỉ có tại LuatVietnam.vn. Nội dung hợp nhất tổng hợp lại tất cả các quy định còn hiệu lực của văn bản gốc và các văn bản sửa đổi, bổ sung, đính chính... trên một trang. Việc hợp nhất văn bản gốc và những văn bản, Thông tư, Nghị định hướng dẫn khác không làm thay đổi thứ tự điều khoản, nội dung.
Khách hàng chỉ cần xem Nội dung hợp nhất là có thể nắm bắt toàn bộ quy định hiện hành đang áp dụng, cho dù văn bản gốc đã qua nhiều lần chỉnh sửa, bổ sung.
- Tải về
Quyết định 468/QĐ-BYT Hướng dẫn phòng và kiểm soát lây nhiễm bệnh viêm đường hô hấp cấp
| Cơ quan ban hành: | Bộ Y tế |
Số công báo:
Số công báo là mã số ấn phẩm được đăng chính thức trên ấn phẩm thông tin của Nhà nước. Mã số này do Chính phủ thống nhất quản lý.
|
Đang cập nhật |
| Số hiệu: | 468/QĐ-BYT | Ngày đăng công báo: | Đang cập nhật |
| Loại văn bản: | Quyết định | Người ký: | Nguyễn Trường Sơn |
|
Ngày ban hành:
Ngày ban hành là ngày, tháng, năm văn bản được thông qua hoặc ký ban hành.
|
19/02/2020 |
Ngày hết hiệu lực:
Ngày hết hiệu lực là ngày, tháng, năm văn bản chính thức không còn hiệu lực (áp dụng).
|
Đã biết
|
|
Áp dụng:
Ngày áp dụng là ngày, tháng, năm văn bản chính thức có hiệu lực (áp dụng).
|
Đã biết
|
Tình trạng hiệu lực:
Cho biết trạng thái hiệu lực của văn bản đang tra cứu: Chưa áp dụng, Còn hiệu lực, Hết hiệu lực, Hết hiệu lực 1 phần; Đã sửa đổi, Đính chính hay Không còn phù hợp,...
|
Đã biết
|
| Lĩnh vực: | Y tế-Sức khỏe COVID-19 |
TÓM TẮT QUYẾT ĐỊNH 468/QĐ-BYT
Theo khuyến cáo của Bộ Y tế, tất cả các người bệnh và nhân viên y tế khi có triệu chứng đường hô hấp cần phải áp dụng nguyên tắc vệ sinh hô hấp, bao gồm: Che miệng mũi bằng khăn giấy khi ho và hắt hơi, sau đó bỏ ngay khăn giấy trong thùng chất thải. Trong trường hợp không có khăn giấy có thể ho vào mặt trên của khuỷu tay, không dùng bàn tay che miệng khi ho.
Người bệnh khi có triệu chứng hắt hơi cần mang khẩu trang y tế khi tiếp xúc gần (< 2m), hoặc nhân viên y tế khi thăm khám bệnh nhân có nguy cơ lây nhiễm COVID-19 qua đường giọt bắn. Đồng thời rửa tay khi tiếp xúc với chất bài tiết. Đứng hoặc ngồi cách xa người nhiễm hoặc nghi ngờ nhiễm COVID-19 ít nhất 2m.
Đối với người không có triệu chứng hô hấp nên tránh tụ tập hoặc đến nơi đông đúc; duy trì khoảng cách ít nhất 2m với bất kỳ người nào có triệu chứng ho, hắt hơi…..Đồng thời thường xuyên vệ sinh tay bằng dung dịch chứa cồn nếu tay không dính bẩn hoặc bằng xà phòng và nước khi tay dính bẩn.
Người có triệu chúng hô hấp nên đeo khẩu trang y tế và đi khám càng sớm càng tốt nếu bị sốt, ho, khó thở… sử dụng và quản lý khẩu trang đúng để đảm bảo có hiệu quả và tránh nguy cơ lây truyền liên quan tới việc sử dụng và thải bỏ khẩu trang không đúng cách.
Các hướng dẫn trên được ban hành kèm theo Quyết định 468/QĐ-BYT ngày 19/02/2020 hướng dẫn phòng và kiểm soát lây nhiễm bệnh viêm đường hô hấp cấp do vi rút Corona 2019 (COVID-19) trong các cơ sở khám bệnh, chữa bệnh, có hiệu lực thi hành kể từ ngày kể từ ngày ký ban hành.
Văn bản này được thay thế bởi 5188/QĐ-BYT
Xem chi tiết Quyết định 468/QĐ-BYT có hiệu lực kể từ ngày 19/02/2020
Tải Quyết định 468/QĐ-BYT
 Quyết định 468/QĐ-BYT PDF (Bản có dấu đỏ)
Quyết định 468/QĐ-BYT PDF (Bản có dấu đỏ) Quyết định 468/QĐ-BYT DOC (Bản Word)
Quyết định 468/QĐ-BYT DOC (Bản Word)|
BỘ Y TẾ |
CỘNG HÒA XÃ HỘI CHỦ NGHĨA VIỆT NAM |
|
Số: 468/QĐ-BYT |
Hà Nội, ngày 19 tháng 02 năm 2020 |
QUYẾT ĐỊNH
VỀ VIỆC BAN HÀNH HƯỚNG DẪN PHÒNG VÀ KIỂM SOÁT LÂY NHIỄM BỆNH VIÊM ĐƯỜNG HÔ HẤP CẤP DO VI RÚT CORONA 2019 (COVID-19) TRONG CÁC CƠ SỞ KHÁM BỆNH, CHỮA BỆNH
---------
BỘ TRƯỞNG BỘ Y TẾ
Căn cứ Nghị định số 75/2017/NĐ-CP ngày 20 tháng 6 năm 2017 của Chính phủ quy định chức năng, nhiệm vụ, quyền hạn về cơ cấu tổ chức của Bộ Y tế;
Xét đề nghị của Cục trưởng Cục Quản lý Khám, chữa bệnh, Bộ Y tế,
QUYẾT ĐỊNH:
Điều 1. Ban hành kèm theo Quyết định này “Hướng dẫn phòng và kiểm soát lây nhiễm bệnh viêm đường hô hấp cấp do vi rút Corona 2019 (COVID-19) trong các cơ sở khám bệnh, chữa bệnh”.
Điều 2. Quyết định này có hiệu lực kể từ ngày ký, ban hành.
Điều 3. Các Ông, Bà: Chánh văn phòng Bộ; Chánh Thanh tra Bộ; Vụ trưởng Cục trưởng các Vụ, Cục thuộc Bộ Y tế; Giám đốc Sở Y tế các tỉnh, thành phố trực thuộc Trung ương; Giám đốc Bệnh viện, Viện nghiên cứu có giường bệnh trực thuộc Bộ Y tế; Thủ trưởng Y tế các Bộ, Ngành và Thủ trưởng các đơn vị có liên quan chịu trách nhiệm thi hành Quyết định này./.
|
Nơi nhận: |
KT. BỘ TRƯỞNG |
Các nội dung về quản lý chất thải y tế, vệ sinh trong phòng, chống dịch COVID-19 và các nội dung liên quan tại “Hướng dẫn phòng và kiểm soát lây nhiễm bệnh viêm đường hô hấp cấp do vi rút Corona 2019 (COVID-19) trong các cơ sở khám bệnh, chữa bệnh” ban hành kèm theo Quyết định số 468/QĐ-BYT được thay thế theo quy định tại Điều 3 Quyết định số 3455/QĐ-BCĐQG.
HƯỚNG DẪN
PHÒNG VÀ KIỂM SOÁT LÂY NHIỄM BỆNH VIÊM ĐƯỜNG HÔ HẤP CẤP DO VI RÚT CORONA 2019 (COVID-19) TRONG CƠ SỞ KHÁM BỆNH, CHỮA BỆNH
(Kèm theo Quyết định số 468/QĐ-BYT ngày 19 tháng 02 năm 2020 của Bộ trưởng Bộ Y tế)
|
DANH MỤC TỪ VIẾT TẮT |
|
|
BYT: |
Bộ Y tế |
|
KBCB: |
Khám bệnh, chữa bệnh |
|
KSNK: |
Kiểm soát nhiễm khuẩn |
|
NB: |
Người bệnh |
|
COVID-19: |
Vi rút Corona 2019 gây viêm đường hô hấp cấp |
|
NVYT: |
Nhân viên y tế |
|
PHCN: |
Phòng hộ cá nhân |
|
PNC: |
Phòng ngừa chuẩn |
|
XN: |
Xét nghiệm |
MỤC LỤC
Danh mục từ viết tắt
Giải thích từ ngữ
Chiến lược, nguyên tắc và biện pháp kiểm soát lây nhiễm COVID-19
Tổ chức sàng lọc, tiếp nhận và cách ly người nhiễm hoặc nghi ngờ nhiễm COVID-19
Hướng dẫn xây dựng khu cách ly trong cơ sở khám bệnh, chữa bệnh
Sử dụng phương tiện phòng hộ cá nhân
Vệ sinh tay
Xử lý dụng cụ
Xử lý đồ vải
Xử lý dụng cụ ăn uống
Vệ sinh khử khuẩn bề mặt môi trường
Vệ sinh phương tiện vận chuyển người nhiễm hoặc nghi ngờ nhiễm COVID-19
Xử lý chất thải
Lấy, bảo quản, đóng gói và vận chuyển bệnh phẩm
Phòng ngừa lây nhiễm trong xét nghiệm COVID-19
Xử lý thi hài người nhiễm hoặc nghi ngờ nhiễm COVID-19
Hướng dẫn phòng ngừa lây nhiễm COVID-19 cho người nhà và khách thăm
Phụ lục
Tài liệu tham khảo
GIẢI THÍCH TỪ NGỮ
Trong phạm vi của Hướng dẫn này, các từ ngữ dưới đây được hiểu như sau:
Buồng đệm (Anteroom): là buồng nhỏ nằm giữa hành lang và buồng cách ly, là nơi chuẩn bị các phương tiện cần thiết cho buồng cách ly.
Nhân viên y tế (Health care worker): là tất cả nhân viên, người lao động trong cơ sở khám bệnh, chữa bệnh có liên quan đến khám, điều trị, chăm sóc người bệnh (bao gồm bác sĩ, điều dưỡng, kỹ thuật y, nhân viên vật lý trị liệu, nhân viên xã hội, tâm lý, dược sĩ, nhân viên vệ sinh...).
Lây truyền qua đường tiếp xúc (Contact transmission): là phương thức lây truyền phổ biến nhất. Lây truyền qua đường tiếp xúc chia thành 2 nhóm:
- Lây truyền qua đường tiếp xúc trực tiếp: vi sinh vật được truyền từ người này sang người khác do sự tiếp xúc trực tiếp giữa mô hoặc tổ chức của cơ thể (gồm cả da và niêm mạc) người này với da, niêm mạc người khác mà không thông qua vật trung gian hoặc người trung gian bị nhiễm.
- Lây truyền qua đường tiếp xúc gián tiếp thông qua các vật dụng bị ô nhiễm.
Lây truyền qua đường tiếp xúc là đường lây truyền chủ yếu nhất làm lan truyền vi sinh vật từ người bệnh (NB) này sang NB khác hay từ nhân viên y tế (NVYT) sang NB và ngược lại.
Nhân viên y tế có những hoạt động tiếp xúc trực tiếp hoặc gián tiếp với NB, với máu hoặc dịch cơ thể từ NB có nguy cơ nhiễm bệnh hoặc làm lan truyền bệnh trong cơ sở khám bệnh, chữa bệnh (KBCB).
Lây truyền qua đường giọt bắn (Droplet transmission): lây truyền qua đường giọt bắn xảy ra khi niêm mạc của người nhận (niêm mạc mũi, kết mạc và ít gặp hơn là niêm mạc miệng) gặp phải những giọt bắn mang tác nhân gây bệnh có kích thước ≥ 5μm. Các hạt này chứa các vi sinh vật gây bệnh tạo ra khi ho, hắt hơi, nói chuyện hoặc khi thực hiện một số thủ thuật (hút, đặt nội khí quản, vật lý trị liệu lồng ngực, hồi sức tim phổi...). Lây truyền qua giọt bắn khi có tiếp xúc gần (< 2 mét giữa NB và người tiếp xúc gần). Các tác nhân gây bệnh lây truyền theo giọt bắn thường gặp như: vi sinh vật gây viêm phổi, ho gà, bạch hầu, cúm, SARS, quai bị, Ebola, COVID-19...
Phơi nhiễm do nghề nghiệp (Occupational exposure): là thuật ngữ để chỉ sự tiếp xúc trực tiếp của niêm mạc hay da không nguyên vẹn với máu, mô hay các dịch cơ thể có chứa nguồn bệnh lây nhiễm hoặc tiếp xúc trực tiếp với nguồn hóa chất, các tia có hại cho cơ thể trong quá trình làm việc của NVYT. Phơi nhiễm nghề nghiệp có thể xảy ra qua da bị tổn thương (kim hoặc vật sắc nhọn xuyên qua da), tiếp xúc với màng nhầy (ví dụ như mắt, mũi hoặc miệng) và tiếp xúc với da không còn nguyên vẹn.
Phòng ngừa chuẩn (Standard precaution): là tập hợp các biện pháp phòng ngừa cơ bản áp dụng cho tất cả NB trong các cơ sở KBCB không phụ thuộc vào chẩn đoán, tình trạng nhiễm trùng và thời điểm chăm sóc dựa trên nguyên tắc coi tất cả máu, chất tiết, chất bài tiết (trừ mồ hôi) đều có nguy cơ lây truyền bệnh. Phòng ngừa chuẩn cần được áp dụng khi chăm sóc, điều trị cho tất cả NB trong cơ sở KBCB, không phụ thuộc vào chẩn đoán và tình trạng nhiễm trùng của NB.
Phòng ngừa dựa trên đường lây truyền (Transmission-based precaution): là các biện pháp phòng ngừa lây nhiễm qua 3 đường chính trong quá trình khám bệnh, chữa bệnh gồm: qua đường tiếp xúc, đường giọt bắn và đường không khí.
Phương tiện phòng hộ cá nhân (Personal Protective Equipment): là những phương tiện cần mang để bảo vệ NVYT khỏi bị nhiễm bệnh khi tiếp xúc gần với NB. Phương tiện phòng hộ cá nhân (PHCN) cũng có thể bảo vệ NB không bị nhiễm các vi sinh vật thường trú và vãng lai từ NVYT. Các phương tiện PHCN thường được sử dụng gồm: găng tay, khẩu trang các loại, áo choàng, tạp dề chống thấm, mũ, kính bảo hộ, tấm che mặt và ủng hay bao giày... Tùy theo nguy cơ về đường lây truyền của bệnh nguyên mà lựa chọn phương tiện PHCN phù hợp.
Vệ sinh tay: Vệ sinh tay (VST) bao gồm các kỹ thuật VST bằng xà phòng với nước sạch hoặc VST với các dung dịch có chứa cồn hoặc dung dịch có chứa cồn và chất khử khuẩn.
Thủ thuật tạo khí dung: là những thủ thuật trong khám bệnh, chữa bệnh có thể làm cho dịch đường hô hấp của người bệnh trở thành các hạt khí dung như nội soi phế quản, đặt nội khí quản, mở khí quản, hồi sức tim phổi, thông khí không xâm lấn.... Các hạt này có khả năng tồn tại trong môi trường không khí.
Số lượng khí thay đổi mỗi giờ hoặc tốc độ thay đổi không khí (Air change per hour - ACH hoặc ACPH): là số lần tổng lượng không khí của một khu vực nhất định (thường là một phòng, một khu vực giới hạn) được lưu thông trong một giờ. Nếu không khí trong không gian là đồng nhất hoặc hỗn hợp hoàn hảo, không khí thay đổi mỗi giờ là thước đo số lần không khí trong một không gian xác định được thay thế.
Ví dụ ACH=12 của một phòng có thể tích 30 m3 là số lượng khí ra vào phòng đó trong một giờ đạt 30 m3 x 12 = 360m3.
Khẩu trang y tế (Medical mask hoặc Surgical mask): Khẩu trang được các NVYT sử dụng hàng ngày trong các cơ sở khám bệnh, chữa bệnh mang khi làm thủ thuật, phẫu thuật hoặc khi tiếp xúc với NB có thể lây truyền qua giọt bắn, hô hấp. Khẩu trang y tế còn có thể gọi là khẩu trang ngoại khoa hay khẩu trang phẫu thuật. Tại Việt Nam, tiêu chuẩn khẩu trang y tế được qui định theo Bộ TCVN 8389-2010 gồm các loại theo tiêu chuẩn sau:
- TCVN 8389-1:2010: Khẩu trang y tế thông thường.
- TCVN 8389-2:2010: Khẩu trang y tế phòng nhiễm khuẩn.
- TCVN 8389-3:2010: Khẩu trang y tế phòng độc hóa chất.
Trong hướng dẫn này, khẩu trang y tế được hiểu là khẩu trang đạt TCVN 8389-2 hoặc tương đương.
Khẩu trang có hiệu lực lọc cao (Respirators mask): trong hướng dẫn này, khái niệm khẩu trang có hiệu lực lọc cao được hiểu là loại khẩu trang đạt chứng nhận N95 theo tiêu chuẩn của Viện an toàn và sức khỏe nghề nghiệp quốc gia Hoa Kỳ (NIOSH) hoặc tiêu chuẩn FFP2 của Liên minh châu Âu (EU) hoặc tương đương (sau đây gọi chung là khẩu trang N95).
CHIẾN LƯỢC, NGUYÊN TẮC VÀ BIỆN PHÁP KIỂM SOÁT LÂY NHIỄM COVID-19
1. Đại cương về vi rút Corona và COVID-19
Vi rút Corona (CoV) là một họ vi rút lớn ở động vật và người. Họ vi rút Corona được chia làm 4 giống, bao gồm 2 giống anpha và 2 giống beta gây bệnh trên người, với các triệu chứng từ cảm thông thường đến những trường hợp bệnh nghiêm trọng hơn. Có khoảng 30% các trường hợp nhiễm trùng đường hô hấp trên gây nên bởi 229E và OC43 từ giống alpha-CoV và NL63, HKU1 từ giống beta- CoV. Giống beta Corona là nguyên nhân của hội chứng viêm đường hô hấp cấp tính nặng SARS-CoV và hội chứng bệnh hô hấp Trung Đông (MERS-CoV), gây viêm phổi nặng có thể dẫn tới tử vong.
Vi rút Corona có hình cầu với đường kính khoảng 125nm, có các protein bề mặt nổi lên hình gai. Vi rút chứa 4 protein cấu trúc chính là protein gai (S), protein màng (M), protein vỏ (E) và nucleocapsid (N). Bên trong vỏ của virion là nucleocapsid sợi đơn dương, đối xứng xoắn ốc. Vi rút có RNA sợi đơn dương tính, không phân đoạn, khoảng 30 kb.
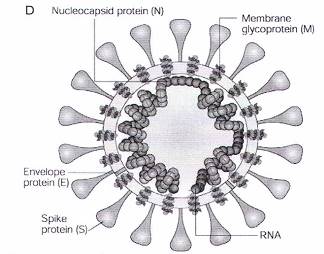
Hình 1: Cấu trúc vi rút Corona
Vào tháng 4 năm 2012 tại Ả Rập Xê út, một NB nhập viện vì viêm phổi, tổn thương thận cấp tính và sau đó tử vong. Đây là trường hợp đầu tiên được xác định nhiễm và tử vong do một chủng vi rút mới. Trong thời gian ngắn sau đó, xuất hiện nhiều NB khác cũng có các triệu chứng tương tự và có cùng tiền sử ở hoặc đi qua Ả Rập Xê Út. Tác nhân gây bệnh sau đó được xác định là một chủng vi rút: Corona hoàn toàn mới gây ra hội chứng viêm đường hô hấp và được đặt tên là Hội chứng viêm đường hô hấp cấp vùng Trung Đông (viết tắt là MERS-CoV: Middle East Respiratory Syndrome of Coronavirus) và được xếp vào là bệnh truyền nhiễm nhóm A. Dịch do MERS-CoV gây ra đã khiến 2.494 trường hợp mắc, 858 trường hợp tử vong (tính đến 12/2015) tại 27 quốc gia, trong đó Trung quốc là nơi có ca bệnh thứ phát do lây truyền từ người sang người.
Nguồn gốc của MERS-CoV chưa được hiểu đầy đủ, một số giả thiết cho rằng có thể có nguồn gốc từ dơi và được truyền cho lạc đà. Người mắc bệnh thường có những triệu chứng của viêm đường hô hấp cấp tính: sốt, ho, viêm phổi nặng và nhanh chóng dẫn đến suy hô hấp cấp, ngoài ra có thể kèm theo các triệu chứng đường tiêu hóa như tiêu chảy và có thể gây suy tạng đặc biệt là suy thận. Tỷ lệ tử vong lên tới 40%. Cho đến nay, bệnh chưa có thuốc điều trị đặc hiệu và vắc xin.
Cuối năm 2019, tại Trung Quốc, bùng phát bệnh viêm phổi Trung Quốc, còn được gọi là bùng phát dịch viêm phổi Vũ Hán do một chủng vi rút Corona gây ra. Dịch bắt đầu vào giữa tháng 12/2019 tại thành phố Vũ Hán, khi một nhóm người bị viêm phổi không rõ nguyên nhân, được liên kết chủ yếu với người làm việc tại chợ hải sản Hoa Nam. Các nhà khoa học Trung Quốc sau đó đã phân lập được một loại vi rút Corona hoàn toàn mới (ban đầu WHO ký hiệu là 2019-nCoV, sau đó chính thức đặt tên là COVID-19), được phát hiện có trình tự gen giống ít nhất 70% với SARS-CoV.
Các ca nghi ngờ đầu tiên được báo cáo vào ngày 31/12/2019, với các triệu chứng đầu tiên xuất hiện vào ngày 08/12/2019. Hiện nay bệnh dịch COVID-19 đang có diễn biến rất phức tạp. Tính đến hết ngày 18/02/2020 trên thế giới đã có 73.335 người mắc, 1.874 người tử vong, chủ yếu tại vùng tâm điểm của dịch, thành phố Vũ Hán, tỉnh Hồ Bắc, Trung Quốc. Trên thế giới, 28 quốc gia và vùng lãnh thổ khác đã thông báo có người nhiễm COVID-19 như Hồng Kông, Ma Cao, Philipines, Camphuchia, Thái Lan, Singapore, Malaysia, Sri Lanka, Ấn Độ, Nepal, UAE, Nhật Bản, Hàn Quốc, Đài Loan, Úc, Đức, Pháp, Tây Ban Nha, Italy, Anh, Thụy Điển, Phần Lan, Bỉ, Nga, Mỹ, Canada, Ai Cập và Việt Nam; đã xác định có sự lây truyền từ người sang người.
Tại Việt Nam, đến ngày 18/02/2020 đã có 16 người xác định nhiễm COVID- 19. Ban đầu có 02 trường hợp người Trung Quốc được xác định nhiễm COVID-19 (người bố đến từ thành phố Vũ Hán và lây nhiễm cho người con đang sinh sống và làm việc tại Việt Nam. Hiện cả hai đã khỏi và xuất viện); 06 người Việt Nam trở về từ Vũ Hán (05 người đã khỏi và xuất viện, 01 người đã khỏi và theo dõi tiếp); 06 người Việt Nam có tiếp xúc gần với người dương tính với COVID-19 (02 người đã khỏi và xuất viện, 01 người đã khỏi và theo dõi tiếp); 01 người Mỹ đến Việt Nam, trước đó có quá cảnh tại Vũ Hán, Trung Quốc; 01 trẻ 03 tháng tuổi có tiếp xúc gần với người dương tính với COVID-19.
COVID-19 chủ yếu lây truyền qua đường giọt bắn trong phạm vi gần với người nhiễm COVID-19 và qua đường tiếp xúc, do vậy mang khẩu trang y tế, VST và vệ sinh bề mặt môi trường là các biện pháp tối quan trọng trong phòng ngừa lây nhiễm. Áp dụng các biện pháp phòng ngừa lây truyền qua đường không khí tại các khu vực có thực hiện các thủ thuật tạo ra khí dung, đặc biệt trong phạm vi gần (<2 mét) và trong khu vực kín, thông khí kém.
2. Các định nghĩa ca bệnh:
2.1. Trường hợp bệnh nghi ngờ: bao gồm các trường hợp:
A. Người bệnh có sốt và viêm đường hô hấp cấp tính VÀ không lý giải được bằng các căn nguyên khác VÀ có tiền sử đến/ở/đi về từ vùng dịch tễ có bệnh do 2019-nCoV trong khoảng 14 ngày trước khi khởi phát các triệu chứng. HOẶC:
B. Người bệnh có bất kỳ triệu chứng hô hấp nào VÀ có ít nhất một trong hai yếu tố dịch tễ sau, xuất hiện trong khoảng 14 ngày trước khi khởi phát các triệu chứng:
a. Tiếp xúc gần (*) với trường hợp bệnh có thể hoặc xác định nhiễm COVID-19.
b. Làm việc hoặc có mặt tại các cơ sở y tế đang điều trị các ca bệnh viêm đường hô hấp cấp tính đã xác định hoặc có thể nhiễm COVID-19 VÀ tiếp xúc trực tiếp với những người bệnh này.
* Tiếp xúc gần bao gồm:
- Tiếp xúc tại các cơ sở y tế, bao gồm: trực tiếp chăm sóc người bệnh nhiễm COVID-19; làm việc cùng với nhân viên y tế nhiễm COVID-19; tới thăm người bệnh hoặc ở cùng phòng bệnh có người bệnh nhiễm COVID-19.
- Tiếp xúc trực tiếp trong khoảng cách ≤ 1-2 mét với trường hợp bệnh nghi ngờ hoặc xác định nhiễm COVID-19.
- Sống cùng nhà với trường hợp bệnh nghi ngờ hoặc xác định nhiễm COVID-19
- Làm việc cùng phòng, học cùng lớp, sinh hoạt chung... với trường hợp bệnh nghi ngờ hoặc xác định nhiễm COVID-19.
- Di chuyển trên cùng phương tiện với trường hợp bệnh nghi ngờ hoặc xác định nhiễm COVID-19.
2.2. Trường hợp bệnh có thể:
Là các trường hợp bệnh nghi ngờ nhưng không thể lấy bệnh phẩm xét nghiệm hoặc chưa có kết quả xét nghiệm khẳng định.
2.3. Trường hợp bệnh xác định:
Là trường hợp bệnh nghi ngờ hoặc có thể đã được khẳng định bằng xét nghiệm real-time RT-PCR dương tính với COVID-19 hoặc bằng kỹ thuật giải trình tự gene.
3. Chiến lược phòng ngừa COVID-19
Chiến lược kiểm soát nhiễm khuẩn (KSNK) nhằm ngăn chặn hoặc hạn chế lây lan COVID-19 trong các cơ sở khám bệnh, chữa bệnh bao gồm:
- Áp dụng các biện pháp PNC đối với tất cả người bệnh.
- Nhận biết sớm, cách ly và kiểm soát nguồn lây nhiễm.
- Thực hiện áp dụng các biện pháp phòng ngừa chuẩn (PNC), cần áp dụng phòng ngừa lây truyền qua đường giọt bắn và qua đường tiếp xúc. Áp dụng các biện pháp phòng ngừa lây truyền qua đường không khí trong khu vực thực hiện các thủ thuật tạo khí dung.
- Các biện pháp hành chính.
- Kiểm soát môi trường và kỹ thuật.
4. Nguyên tắc phòng ngừa
- Thực hiện PNC kết hợp với phòng ngừa qua đường tiếp xúc và đường giọt bắn trong thăm khám, chăm sóc người nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Trong chăm sóc người nhiễm hoặc nghi ngờ nhiễm COVID-19 có thực hiện thủ thuật có tạo khí dung, bổ sung các biện pháp phòng ngừa lây truyền qua đường không khí.
- Thực hiện vệ sinh hô hấp đối với tất cả NB có triệu chứng về đường hô hấp.
- Kiểm soát tốt thông khí, môi trường, VST, mang đầy đủ các phương tiện PHCN là biện pháp quan trọng nhất trong phòng ngừa lây nhiễm cho NVYT.
5. Các biện pháp kiểm soát lây truyền trong cơ sở khám bệnh, chữa bệnh
5.1. Phòng ngừa chuẩn
Phòng ngừa chuẩn là tập hợp các biện pháp phòng ngừa cơ bản áp dụng cho tất cả NB trong các cơ sở KBCB không phụ thuộc vào chẩn đoán, tình trạng nhiễm trùng và thời điểm chăm sóc của NB, dựa trên nguyên tắc coi tất cả máu, chất tiết, chất bài tiết (trừ mồ hôi) đều có nguy cơ lây truyền bệnh. Phòng ngừa chuẩn bao gồm các biện pháp sau:
- Vệ sinh tay theo 5 thời điểm VST và theo kỹ thuật VST 6 bước.
- Sử dụng phương tiện PHCN phù hợp tùy theo tình huống như khi xử lý máu, dịch tiết, chất tiết hay khi dự kiến sẽ tiếp xúc với máu, dịch tiết, chất tiết.
- Thực hiện quy tắc vệ sinh hô hấp khi ho, hắt hơi.
- Thực hiện dự phòng tổn thương do vật sắc nhọn trong khi chăm sóc NB.
- Xử lý dụng cụ chăm sóc NB tái sử dụng đúng quy trình.
- Thu gom, vận chuyển, xử lý đồ vải bẩn, an toàn.
- Vệ sinh môi trường chăm sóc NB.
- Xử lý chất thải đúng quy định.
- Sắp xếp NB an toàn.
+ Xếp người bệnh nhiễm COVID-19 có tình trạng bệnh nặng vào phòng cấp cứu khu cách ly hoặc phòng cách ly có đầy đủ phương tiện cấp cứu riêng biệt.
+ Xếp người bệnh không có biểu hiện nặng vào buồng riêng hoặc có thể sắp xếp theo nhóm cùng bệnh chung buồng.
+ Không xếp người có xét nghiệm COVID-19 (+) với những người nghi ngờ nhiễm COVID-19.
5.2. Phòng ngừa dựa theo đường lây truyền
a) Phòng ngừa lây truyền qua đường tiếp xúc (Contact Precautions)
Phòng ngừa lây truyền qua đường tiếp xúc chú ý các điểm:
- Cho NB nằm buồng riêng. Nếu không có buồng riêng, xếp NB ở cùng phòng với NB nhiễm cùng tác nhân gây bệnh.
- Mang găng sạch khi vào phòng cách ly. Trong quá trình chăm sóc NB cận thay găng sau khi tiếp xúc với vật dụng có khả năng chứa nồng độ vi rút, vi khuẩn cao (phân, dịch dẫn lưu, dịch tiết...).
- Mang áo choàng và bao giày sạch khi vào phòng NB và cởi ra trước khi ra khỏi phòng đệm. Sau khi đã cởi áo choàng và bao giầy, phải chú ý không được để áo quần chạm vào bề mặt môi trường hay những vật dụng khác.
- Tháo găng, áo choàng trước khi ra khỏi phòng và vệ sinh tay ngay bằng dung dịch khử khuẩn. Sau khi đã tháo găng và VST, không được sờ vào bất cứ bề mặt môi trường hay vật dụng nào trong phòng đệm.
- Hạn chế tối đa việc vận chuyển NB. Cố gắng sử dụng các kỹ thuật tại giường (X-quang, siêu âm...), nếu cần phải vận chuyển thì phải thông báo nơi chuyển đến, trước khi chuyển, cho NB mang khẩu trang y tế trong quá trình vận chuyển, trong trường hợp có tổn thương da phải che phủ tránh phát tán nguồn nhiễm, sử dụng các lối đi vận chuyển riêng được xác định trước để giảm thiểu phơi nhiễm cho NVYT, NB khác và người khác.
- Dụng cụ, thiết bị chăm sóc NB: Nên sử dụng một lần cho từng NB riêng biệt. Nếu không thể, cần làm sạch, khử khuẩn và tiệt khuẩn trước khi sử dụng cho NB khác.
b) Phòng ngừa lây truyền qua đường giọt bắn (Droplet Precautions)
Phòng ngừa lây truyền qua đường giọt bắn cần chú ý các điểm sau:
- Cho NB nằm phòng riêng. Nếu không có phòng riêng, xếp NB ở cùng phòng với NB nhiễm cùng tác nhân gây bệnh. Có thể xếp chung với NB khác nhưng phải giữ khoảng cách xa thích hợp tối thiểu trên 2 mét.
- Mang khẩu trang y tế, kính bảo vệ mắt hoặc mạng che mặt nhất là với những thao tác cần tiếp xúc gần với NB.
- Hạn chế tối đa vận chuyển NB, nếu cần phải vận chuyển thì phải cho NB mang khẩu trang y tế, sử dụng lối đi riêng để vận chuyển người bệnh nhằm tránh lây nhiễm cho NVYT, NB khác và người khác.
c) Phòng ngừa lây truyền qua đường không khí (Airborne Precautions)
Khi thực hiện các thủ thuật có tạo khí dung trên người nhiễm COVID-19 cần áp dụng các biện pháp phòng ngừa lây truyền qua đường không khí.
Việc xử lý không khí và thông khí phòng bệnh là cần thiết để ngăn ngừa sụ: lan truyền bệnh.
Những biện pháp phòng ngừa lây truyền qua đường không khí bao gồm:
- Xếp NB nằm phòng riêng. Trường hợp không thể bố trí phòng riêng cần sắp xếp NB cùng nhóm đã xác định nhiễm hoặc nhóm nghi ngờ nhiễm chung phòng.
- Đảm bảo thông khí an toàn: thông khí tự nhiên, thông khí cơ học hoặc phối hợp nhưng lưu lượng không khí trao đổi tối thiểu phải đạt ≥12 luồng khí/giờ. Cơ thể dùng hệ thống hút khí ra ngoài (thấp bên dưới, cách nên nhà 10-15cm) ra khu vực không có người qua lại và tránh cho không khí đã ô nhiễm tái lưu thông.
- Bất kỳ người nào vào phòng cách ly phải mang khẩu trang có hiệu lực lọc cao (ví dụ khẩu trang N95).
- Hạn chế vận chuyển NB. Chỉ vận chuyển trong những trường hợp hết sức cần thiết. Mang khẩu trang y tế cho NB khi ra khỏi phòng.
- Tiến hành thủ thuật trong phòng đơn với cửa ra vào phải đóng kín, thông khí an toàn và cách xa những NB khác.
- Lựa chọn dụng cụ và phương pháp hút đờm kín cho NB có thông khí hỗ trợ nếu có chỉ định hút đờm.
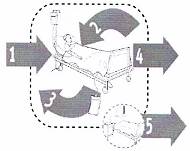
5.3. Tuân thủ nghiêm ngặt quy tắc vệ sinh hô hấp
Nguyên tắc của khuyến cáo vệ sinh hô hấp như sau:
- Tất cả những NB hoặc NVYT khi có triệu chứng đường hô hấp cần phải áp dụng nguyên tắc vệ sinh hô hấp, bao gồm:
+ Che miệng mũi bằng khăn giấy khi ho và hắt hơi, sau đó bỏ ngay khăn giấy trong thùng chất thải.
+ Trong trường hợp không có khăn giấy có thể ho vào mặt trên của khuỷu tay, KHÔNG dùng bàn tay che miệng khi ho.
+ Yêu cầu NB có triệu chứng ho hắt hơi mang khẩu trang y tế khi tiếp xúc gần (< 2m), hoặc NVYT khi thăm khám NB có nguy cơ lây nhiễm COVID-19 qua đường giọt bắn.
+ Rửa tay sau khi tiếp xúc với chất tiết.
+ Đứng hay ngồi cách xa người nhiễm hoặc nghi ngờ nhiễm COVID-19 ít nhất 2 mét.
- Nên treo poster hướng dẫn vệ sinh hô hấp ở những nơi dễ quan sát như khu vực khám bệnh, cách ly.
5.4. Kiểm soát môi trường
5.4.1. Môi trường bề mặt sàn nhà, tường, hàng lang
Kiểm soát môi trường là biện pháp quan trọng trong phòng ngừa lây nhiễm COVID-19. Cần chú ý những nguyên tắc sau:
- Các bề mặt môi trường cần phải được làm sạch và khử khuẩn bằng hóa chất khử khuẩn phù hợp và được cấp phép.
- Những đám máu hoặc các chất thải, chất tiết sinh học như chất nôn, phân có trên các bề mặt môi trường phải được loại bỏ ngay bằng khăn tẩm hóa chất chứa Clo hoạt tính 0,5% (5.000 ppm), sau đó lau sạch bằng khăn sạch và lau lại lần 2 với Clo hoạt tính 0,05%.
Xem chi tiết tại phần Vệ sinh, khử khuẩn môi trường bề mặt
4.5.2. Thông khí
Đảm bảo thông khí thích hợp giữa các khu vực:
- Khu tiếp nhận NB, hành lang, phòng chờ thông thoáng, không cần làm kín.
- Khu vực buồng bệnh:
+ Buồng cách ly tối ưu là áp lực âm.
+ Trường hợp không thể làm phòng áp lực âm, cần sử dụng không khí hỗn hợp hoặc thông khí tự nhiên, đảm bảo thông khí trong buồng cách ly tối thiểu ≥12 luồng không khí trao đổi/giờ.
+ Buồng làm thủ thuật có khả năng tạo khí dung, phải thực hiện trong buồng có thông khí thích hợp (≥12 luồng khí trao đổi/giờ).
+ Nếu không có buồng đạt tiêu chuẩn nói trên:
ü Tiến hành thủ thuật trong buồng cách xa những NB khác. Buồng thủ thuật phải thông khí tốt, ở cuối chiều gió, có cửa sổ đối lưu 2 chiều, cửa sổ mở hướng ra khu vực không có người qua lại.
ü Có thể dùng hệ thống hút khí ra ngoài, khí hút ra phải thải ra môi trường trống, không có người qua lại, không thải vào hành lang hoặc các phòng kế cận.
4.5.3. Phương tiện, máy móc, giường tủ
Vệ sinh và khử khuẩn hàng ngày, ít nhất ngày 2 lần và khi cần (giữa hai NB, khi NB tử vong, chuyển hoặc ra viện) bằng hóa chất khử khuẩn phù hợp và được cấp phép.
Xem chi tiết tại phần Vệ sinh, khử khuẩn môi trường bề mặt.
4.6. Phòng ngừa lây truyền cho cộng đồng
Nhân viên y tế khi chăm sóc người nhiễm hoặc nghi ngờ nhiễm COVID-19, trong giai đoạn đang theo dõi hạn chế tiếp xúc với người thân, cộng đồng cho đến khi hết thời gian nguy cơ, hạn chế phát tán và lây lan trong bệnh viện cũng như cộng đồng.
Cơ sở KBCB cần bố trí một kíp NVYT riêng chăm sóc người nhiễm hoặc nghi ngờ nhiễm COVID-19. Trong quá trình chăm sóc người nhiễm hoặc nghi ngờ nhiễm COVID-19, kíp NVYT này không tham gia chăm sóc những NB khác.
Tuyên truyền cho người dân hạn chế đến những khu vực đang có dịch. Người đã đến những khu vực đó hoặc người có tiếp xúc gần với người đã được khẳng định nhiễm hoặc nghi ngờ nhiễm COVID-19 cần tự cách ly, theo dõi sát thân nhiệt trong vòng 14 ngày. Phải đến bệnh viện ngay khi có sốt hoặc có các triệu chứng về: hô hấp.
Người không có triệu chứng hô hấp nên:
- Tránh tụ tập và thường xuyên đến nơi đông đúc.
- Duy trì khoảng cách ít nhất 2 mét với bất kỳ người nào có triệu chứng hô hấp (ví dụ: ho, hắt hơi).
- Thực hiện VST thường xuyên: bằng dung dịch chứa cồn nếu tay không dính bẩn hoặc bằng xà phòng và nước khi tay bị dính bẩn.
- Nếu ho hoặc hắt hơi che mũi và miệng bằng khuỷu tay gấp hoặc khăn giấy, vứt bỏ khăn giấy ngay sau khi sử dụng và thực hiện VST.
- Hạn chế không chạm vào mắt, mũi và miệng.
Người có triệu chứng hô hấp nên:
- Đeo khẩu trang y tế và đi khám càng sớm càng tốt nếu bị sốt, ho, khó thở...
- Sử dụng và quản lý khẩu trang đúng.
Quản lý khẩu trang:
Nếu đeo khẩu trang y tế, việc sử dụng và thải bỏ phù hợp là điều cần thiết để đảm bảo có hiệu quả và tránh các nguy cơ lây truyền liên quan đến việc sử dụng và thải bỏ khẩu trang không đúng cách.
Việc đeo khẩu trang phải đúng chỉ định và đúng kỹ thuật. Không được lạm dụng. Việc dùng không đúng mục đích có thể làm lây lây mầm bệnh.
Chi tiết hướng dẫn cách đeo và tháo khẩu trang tại phần Sử dụng phương tiện PHCN.
4.7. Các nguyên tắc kiểm soát phòng ngừa khác
Phải kết hợp đồng thời nhiều biện pháp KSNK, bao gồm cả tổ chức quy trình sàng lọc, cách ly, vệ sinh môi trường, quản lý chất thải, sử dụng đúng quy trình mặc và cởi phương tiện PHCN; kiểm soát lây nhiễm trong vận chuyển, giải phẫu và xử lý tử thi, kiểm soát lây nhiễm tại phòng xét nghiệm.
TỔ CHỨC SÀNG LỌC, TIẾP NHẬN VÀ CÁCH LY NGƯỜI NHIỄM HOẶC NGHI NGỜ NHIỄM COVID-19
COVID-19 có nguy cơ lây cao nên công tác sàng lọc, phát hiện sớm, cách ly kịp thời là rất quan trọng. Người nhiễm hoặc nghi ngờ nhiễm COVID-19 phải được cách ly ngay và áp dụng nghiêm ngặt các biện pháp phòng ngừa lây truyền.
1. Mục đích
Sàng lọc NB đến khám nhằm phát hiện và cách ly sớm người nhiễm hoặc nghi ngờ nhiễm COVID-19, qua đó ngăn ngừa nguy cơ lây nhiễm COVID-19 từ NB đến NVYT, đến NB khác và môi trường bệnh viện.
2. Nguyên tắc thực hiện
- Cơ sở KBCB cần xây dựng hệ thống nhận biết và phản ứng nhanh khi có người nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Cơ sở KBCB cần xây dựng kế hoạch sàng lọc, phân loại và quản lý người nhiễm hoặc nghi ngờ nhiễm COVID-19 ngay khi đến khám bệnh.
+ Thực hiện các biện pháp phòng ngừa và kiểm soát nhiễm khuẩn nghiêm ngặt (phòng ngừa chuẩn và phòng dựa theo đường lây truyền).
+ Tổ chức phân loại NB ngay khi đến phòng khám của cơ sở KBCB bằng bảng hỏi sàng lọc.
+ Tổ chức khu vực/phòng khám riêng cho những người bệnh có hay không có biểu hiện bệnh lý hô hấp cấp tính (ho, sốt...) nhưng có yếu tố dịch tễ (người đến hoặc đi qua tỉnh Hồ Bắc, Trung Quốc trong vòng 14 ngày (xem thêm Hướng dẫn tại cơ sở cách ly tập trung để phòng chống dịch bệnh viêm đường hô hấp cấp do chủng COVID-19 ban hành theo Quyết định số 344/QĐ-BYT ngày 07/02/2020 của BYT).
+ Khi phát hiện người nhiễm hoặc nghi ngờ nhiễm COVID-19 cần phải khám và cách ly kịp thời (căn cứ vào dấu hiệu bệnh và yếu tố dịch tễ chỉ điểm).
+ Thực hiện khai báo, thông tin, báo cáo ca bệnh theo qui định.
3. Phạm vi áp dụng: Tất cả cơ sở khám bệnh, chữa bệnh.
4. Tổ chức công tác phòng, kiểm soát lây nhiễm COVID-19.
Các cơ sở KBCB cần triển khai thực hiện nghiêm các quy trình, quy định về phòng ngừa và kiểm soát lây nhiễm bệnh dịch do BYT ban hành.
Cần huy động tất cả nguồn lực cho kiểm soát lây nhiễm COVID-19; cứu chữa người mắc bệnh, phòng ngừa lây nhiễm sang NB khác và hạn chế tử vong; chủ động phối hợp với các lực lượng khác khoanh vùng ổ dịch, vận chuyển, cấp cứu, cách ly, điều trị NB, xử lý môi trường ổ dịch kịp thời.
Các cơ sở KBCB cần chủ động chuẩn bị và thực hiện các hoạt động sau:
4.1. Tổ chức, nhân lực
- Thành lập Ban chỉ đạo phòng chống COVID-19 tại các bệnh viện, thành phần gồm: Ban Giám đốc, phòng Kế hoạch tổng hợp, khoa Khám bệnh, khoa Hồi sức cấp cứu, khoa Truyền nhiễm, khoa Nhi, khoa Hô hấp, phòng Hành chính Quản trị, khoa Kiểm soát nhiễm khuẩn, phòng Vật tư Thiết bị y tế, khoa Dược, phòng Điều dưỡng, phòng Tổ chức cán bộ, Y tế cơ quan. Với các bệnh viện tuyên trung ương và tuyến tỉnh/thành phố, Ban chỉ đạo có thể có các tiểu ban điều trị và tiểu ban phòng ngừa lây nhiễm, tiểu ban hậu cần...
- Tùy theo điều kiện thực tế của từng bệnh viện, lãnh đạo bệnh viện quyết định khoa chịu trách nhiệm tiếp nhận điều trị người nhiễm hoặc nghi ngờ nhiễm COVID-19. Khoa chịu trách nhiệm tiếp nhận, sàng lọc, điều trị NB phải có đủ điều kiện để cách ly theo quy chuẩn. Nhân viên làm việc tại khoa này phải được huấn luyện đầy đủ về kiểm soát nhiễm khuẩn, đặc biệt chú ý việc sử dụng phương tiện PHCN theo hướng dẫn để phòng ngừa lây nhiễm trong bệnh viện.
4.2. Tổ chức thu dung và cách ly
- Phân vùng nguy cơ và phân luồng người nhiễm hoặc nghi ngờ nhiễm COVID-19 sẽ di chuyển trong bệnh viện như sau:
+ Vùng nguy cơ cao (màu đỏ) là những khoa chịu trách nhiệm thu dung điều trị ngươi nhiễm hoặc nghi ngờ nhiễm COVID-19 (ví dụ: khu cách ly; khoa Khám bệnh; khoa Hồi sức cấp cứu, khoa Truyền nhiễm, bộ phận xét nghiệm...)
+ Vùng nguy cơ trung bình (màu vàng) là những khoa tiếp nhận NB ho sốt (Ví dụ: buồng khám NB ho sốt khoa Khám bệnh, khoa cấp cứu, khoa Hô hấp, khoa Nhi);
+ Vùng nguy cơ thấp (màu xanh) là những khoa ít có khả năng tiếp nhận khám và điều trị người nhiễm hoặc nghi ngờ nhiễm COVID-19 (Ví dụ: khoa Ngoại, Sản...).
- Việc phân vùng nguy cơ giúp bệnh viện có cơ sở phân công trách nhiệm, triển khai kế hoạch thu dung, điều trị và tập trung nguồn lực còn có hạn cho công tác phòng ngừa (phương tiện, nhân lực, tập huấn, giám sát) cho những vùng có nguy cơ cao.
- Có phương án phân vùng cách ly, bố trí nhân lực, phương tiện... cho những; tình huống dịch lẻ tẻ và tình huống phải tiếp nhận nhiều người nhiễm hoặc nghi ngờ nhiễm COVID-19.
4.3. Điều kiện, phương tiện
4.3.1. Phương tiện vệ sinh tay
Có đầy đủ xà phòng, dung dịch VST có chứa cồn, khăn giấy hoặc khăn lau tay sử dụng 1 lần ở tất cả khu vực cần thiết.
4.3.2. Phòng hộ cá nhân
Áo choàng chống dịch, tạp dề, mũ giấy, khẩu trang y tế, khẩu trang N95, kính (hoặc tấm che mặt), ủng, bao giầy, găng y tế và găng vệ sinh.
4.3.3. Thiết bị
- Thiết bị thông khí hỗ trợ và phương tiện hồi sức cấp cứu khác (máy đo độ bão hòa oxy cầm tay, máy monitor, máy chụp X quang tại giường), oxy và hệ thống tạo, cung cấp oxy, hệ thống hút đờm kín;
- Máy lọc khử khuẩn không khí bằng HEPA.
Để kiểm soát lây nhiễm COVID-19 đạt hiệu quả cao, các phương tiện trên phải luôn sẵn sàng tại mỗi khu vực tiếp nhận và điều trị NB cả khi có và chưa có dịch. Nhân viên y tế phải được huấn luyện, sử dụng thành thạo, hợp lý các phương tiện PHCN và các quy định khác về KSNK bệnh viện.
4.3.4. Hoá chất khử khuẩn, khử khuẩn bề mặt, dụng cụ
Phải lập dự trù, mua sắm và cung cấp đầy đủ hóa chất cho xử lý dụng cụ; vệ sinh khử khuẩn bề mặt môi trường; VST; xử lý chất thải khi có dịch xảy ra.
4.3.5. Phòng cách ly
Các bệnh viện phải triển khai khu vực hoặc phòng cách ly đạt chuẩn theo quy định và luôn sẵn sàng khi có bệnh dịch.
Các cơ sở KBCB khác cần chuẩn bị sẵn khu (phòng) tiếp đón, sàng lọc người nhiễm hoặc nghi ngờ nhiễm COVID-19.
4.3.6. Thuốc
Danh mục thuốc theo phác đồ điều trị.
4.4. Huấn luyện
Cơ sở KBCB phải xây dựng kế hoạch và tổ chức các khóa huấn luyện, đào tạo cho tất cả các NVYT trong cơ sở về kiểm soát lây nhiễm COVID-19. Khoa KSNK chịu trách nhiệm về nội dung, chương trình, tài liệu, phương tiện để hướng dẫn về lý thuyết và thực hành cho nhân viên y tế theo tài liệu của BYT.
4.5. Diễn tập
Ban chỉ đạo phòng chống COVID-19 tại các cơ sở KBCB tổ chức diễn tập nhằm kiểm tra, đánh giá, rút kinh nghiệm những nội dung còn hạn chế để bổ sung, khắc phục và hoàn thiện kế hoạch phòng chống dịch của cơ sở phù hợp với các kế hoạch phòng chống dịch của địa phương, khu vực, quốc gia.
Một số điểm lưu ý trong nội dung diễn tập như sau:
- Kiểm soát sớm: Phân luồng, sàng lọc, phát hiện, chẩn đoán, cách ly sớm, người có triệu chứng nhiễm hoặc nghi ngờ nhiễm COVID-19 tới khám và nhập viện. Thực hiện đúng các quy định liên quan đến vận chuyển NB trong bệnh viện, chuyên khoa, chuyển viện bảo đảm an toàn cho NVYT, nhân viên vận chuyển và cho cộng đồng.
- Bảo đảm các điều kiện cần thiết cho tiếp nhận, điều trị và tổ chức phòng ngừa cách ly trong cơ sở KBCB.
- Bảo đảm NVYT sử dụng đúng phương tiện PHCN, chuẩn bị đủ cơ số phương tiện hiện có và các giải pháp khi nguồn cung cấp phương tiện PHCN bị hạn chế.
- Tuân thủ thực hành PNC và phòng ngừa dựa theo đường lây truyền (qua giọt bắn, qua đường tiếp xúc và có thể qua đường không khí) của NVYT. Bảo đảm sự tuân thủ các quy định, quy trình VST, khử khuẩn, tiệt khuẩn dụng cụ y tế, vệ sinh khử khuẩn khu cách ly và vệ sinh môi trường bệnh viện.
- Thực hành phòng lây nhiễm đối với NVYT, người nhà NB, khách thăm về quản lý chất thải y tế, quản lý đồ vải, dụng cụ ăn uống của NB tại khu vực cách ly, hướng dẫn phòng ngừa lây nhiễm khi NB tử vong.
- Lưu ý phòng ngừa các nhiễm khuẩn bệnh viện khác có liên quan tới chăm sóc người nhiễm hoặc nghi ngờ nhiễm COVID-19 (nhiễm khuẩn phổi, nhiễm khuẩn máu, nhiễm khuẩn tiết niệu...).
4.6. Kiểm tra, giám sát
- Khoa Kiểm soát nhiễm khuẩn chịu trách nhiệm chuyên môn trong kiểm tra giám sát thực hiện kiểm soát lây nhiễm COVID-19; xây dựng quy trình kiểm soát nhiễm khuẩn áp dụng trong bệnh viện, quy trình giám sát thực hiện kiểm soát lây nhiễm trong bệnh viện thông qua Hội đồng KSNK, Ban chỉ đạo chống dịch của bệnh viện trình Giám đốc bệnh viện phê duyệt và tổ chức giám sát việc tuân thủ quy định/quy trình phòng chống dịch và KSNK.
- Phòng Kế hoạch Tổng hợp phối hợp với khoa KSNK giám sát, thống kê, thông báo kịp thời người nhiễm hoặc nghi ngờ nhiễm COVID-19 và những nhân viên y tế có tiếp xúc gần, tổ chức và kiểm tra, giám sát thực hiện các quy định về kiểm soát lây nhiễm.
- Phòng Điều dưỡng phối hợp với khoa KSNK, phòng Kế hoạch Tổng hợp và điều dưỡng trưởng các khoa lâm sàng, kỹ thuật viên trưởng các khoa cận lâm sàng kiểm tra giám sát thực hiện các quy định về kiểm soát lây nhiễm.
4.7. Phân công trách nhiệm và tổ chức thực hiện
Ban Giám đốc, lãnh đạo các khoa/phòng và cá nhân có liên quan chịu trách nhiệm cụ thể các nội dung hoạt động phòng lây nhiễm COVID-19 tại các cơ sở KBCB.
Nội dung kiểm soát lây nhiễm phải được thể hiện trong kế hoạch phòng chống COVID-19 của bệnh viện.
Giám đốc chịu trách nhiệm trang bị đủ cơ sở vật chất, mua sắm thiết bị, vật tư, hoá chất, phương tiện cần thiết phục vụ công tác phòng lây nhiễm. Bố trí khu vực cách ly tại địa điểm thích hợp. Có kế hoạch cải tạo, nâng cấp, xây mới khu cách ly theo đúng hướng dẫn.
4.8. Kinh phí
Kinh phí theo quy định của nhà nước về phòng chống dịch. Thực hiện mua sắm, chi tiêu theo quy định. Trong vụ dịch, khi Bộ Y tế hoặc cơ quan có thẩm quyền công bố dịch, chi tiêu theo quy định phòng chống dịch khẩn cấp.
Giám đốc bệnh viện chịu trách nhiệm bố trí ngân sách và nhân viên chuyên môn cho hoạt động thường xuyên về kiểm soát nhiễm khuẩn. Bệnh viện cần có ngân sách dự phòng cho phòng chống dịch.
5. Sàng lọc, cách ly người nhiễm hoặc nghi ngờ nhiễm COVID-19
5.1. Chuẩn bị cơ sở hạ tầng, phương tiện
- Bố trí, thiết lập khu vực, phòng cách ly bảo đảm yêu cầu cách ly.
- Trang phục PHCN (Xem phần Hướng dẫn sử dụng phương tiện PHCN).
- Phương tiện VST đầy đủ ở tất cả khu vực tiếp nhận NB đến khu vực sàng lọc, khám và điều trị.
- Các dụng cụ, thiết bị và hóa chất khử khuẩn thiết yếu dùng trong chăm sóc, điều trị NB.
- Các phương tiện thu gom chất thải, dụng cụ, đồ vải...
5.2. Các bước thực hiện
Mỗi cơ sở KBCB cần có các khu vực sàng lọc NB ngay từ khu vực phòng khám (Như tại khu vực cổng bảo vệ, các nơi tiếp nhận NB), có ít nhất một phòng khám cách ly các trường hợp ho sốt chưa rõ nguyên nhân đến khám bệnh. Người làm nhiệm vụ phân loại NB phải hướng dẫn cho họ các biện pháp phòng ngừa cách ly ngay khi NB vào khám bệnh.
* Tiến hành chẩn đoán phát hiện sớm người nhiễm hoặc nghi ngờ nhiễm COVID-19 như sau:
- Có yếu tố dịch tễ trong vòng 14 ngày trước khi khởi phát triệu chứng:
+ Người bệnh từ nơi có dịch COVID-19 lưu hành trở về Việt Nam hoặc có tiếp xúc với người đi từ vùng dịch.
+ Tiếp xúc với máu hay dịch cơ thể của NB được xác định hoặc nghi nhiễm COVID-19 tại vùng dịch lưu hành.
+ Đã sống hay đi tới vùng dịch COVID-19 đang lưu hành trong vòng 14 ngày;
+ Trực tiếp xử lý động vật từ các vùng dịch tễ.
- Có biểu hiện lâm sàng của bệnh:
+ Sốt cao đột ngột ≥ 38°C; có thể có đau đầu, đau mỏi cơ.
+ Ho và khó thở.
+ Có biểu hiện viêm phổi hoặc suy hô hấp cấp tính (Xem phần hướng dẫn chẩn đoán nghi ngờ nhiễm COVID-19 của Bộ Y tế, trang 8).
- Khi có những triệu chứng và tiền sử như trên, NB cần được đưa vào khu vực cách ly, cách ly khỏi các NB khác càng sớm càng tốt theo các bước trong Sơ đồ hướng dẫn (Phụ lục 1).
- Trong thời gian có dịch, cần treo các bảng hướng dẫn ngay khu vực ra vào (Cổng bảo vệ) và phòng khám để hướng dẫn NB, người nhà NB có dấu hiệu sốt, ho đến ngay khu vực khám sàng lọc, tránh để họ đi đến các khu vực khác.
- Khu vực buồng đợi, buồng khám, buồng làm thủ thuật cho người nhiễm hoặc nghi ngờ nhiễm COVID-19 phải đảm bảo thông khí tốt, ít nhất nên có trên 12 luồng khí trao đổi mỗi giờ. Có thể thực hiện bằng cách mở toàn bộ cửa sổ, cửa ra vào cùng một hướng trong trường hợp sử dụng thông khí tự nhiên. Nếu bệnh viện sử dụng điều hòa trung tâm thì phải tăng cường số ACH và kiểm tra mức độ an toàn của hệ thống thông khí trung tâm thường xuyên, định kỳ ở các khu vực này.
- Người nhà đi kèm với người nhiễm hoặc nghi ngờ nhiễm COVID-19 cần phải được xem như là có phơi nhiễm với COVID-19 và cũng phải được tâm soát cho đến hết thời gian theo dõi theo quy định để giúp chẩn đoán sớm và phòng ngừa COVID-19 có khả năng gây dịch.
- Trong trường hợp cần vận chuyển, nhân viên vận chuyển phải sử dụng phương tiện PHCN và xe chuyên dụng. Các vật dụng bị ô nhiễm, phương tiện vận chuyển, đồ thải bỏ và chất thải của NB cần phải thu gom và xử lý theo quy định.
* Những lưu ý:
- Người trực tiếp chăm sóc NB phải thực hiện nghiêm ngặt các biện pháp phòng ngừa như: tuân thủ mang phương tiện PHCN; rửa tay ngay bằng xà phòng hoặc dung dịch khử khuẩn khác sau mỗi lần tiếp xúc với NB (xem thêm phần vệ sinh tay và phần mang phương tiện PHCN).
- Người bệnh phải được mang khẩu trang y tế.
- Hạn chế tối đa việc tiếp xúc với NB, vận chuyển NB.
- Thực hiện tốt vệ sinh cá nhân, sử dụng các dung dịch vệ sinh, khử khuẩn đường mũi họng.
- Vệ sinh khử khuẩn phương tiện vận chuyển NB sau mỗi lần sử dụng.
- Lập danh sách những người tiếp xúc gần và theo dõi tình trạng sức khỏe trong vòng 14 ngày kể từ khi tiếp xúc lần cuối. Tư vấn cho người tiếp xúc về các dấu hiệu bệnh và các biện pháp phòng, chống để tự phòng bệnh, tự theo dõi, phát hiện sớm các triệu chứng của người nhiễm hoặc nghi ngờ nhiễm COVID-19. Nếu xuất hiện các triệu chứng của bệnh cần thông báo ngay cho cơ sở y tế gần nhất để được chẩn đoán, điều trị kịp thời.
5.3. Kiểm tra, giám sát
- Khoa KSNK, Phòng Kế hoạch tổng hợp, Phòng Điều dưỡng chịu trách nhiệm kiểm tra, giám sát, huấn luyện việc thực hiện quy trình cách ly của NVYT.
- Nội dung giám sát:
+ Buồng bệnh/khu vực có đạt tiêu chuẩn buồng cách ly.
+ Có đầy đủ phương tiện PHCN theo quy định (quần áo, mũ, khẩu trang, kính, găng tay, ủng...).
+ Ý thức tuân thủ của NVYT về việc thực hiện cách ly theo từng giai đoạn chẩn đoán và điều trị.
- Thực hiện giám sát bằng quan sát trực tiếp và ghi nhận bằng phiếu giám sát.
Thời gian cách ly người nhiễm hoặc nghi ngờ nhiễm COVID-19: Cách ly điều trị tại cơ sở y tế theo hướng dẫn của BYT.
Thông báo trường hợp bệnh:
- Thông báo trong cơ sở y tế theo đúng quy định và phân cấp: Phòng khám/khoa cấp cứu có người nhiễm hoặc nghi ngờ nhiễm COVID-19 cần thông báo ngay cho các đối tượng sau:
+ Bản thân NB và người nhà NB.
+ Thành viên kíp trực (nếu trong giờ trực) hoặc tất cả thành viên trong khoa (trong giờ hành chính).
+ Lãnh đạo bệnh viện và các phòng ban liên quan (Phòng KHTH, khoa KSNK, Phòng Điều dưỡng...).
- Thông báo ra ngoài cơ sở y tế: Cần thông báo bằng văn bản khẩn trong tất cả trường hợp nghi ngờ hoặc xác định cho lãnh đạo y tế cấp trên và cho lãnh đạo cơ quan y tế dự phòng tương đương theo quy định.
Các yếu tố đảm bảo sàng lọc, phát hiện sớm, cách ly kịp thời, điều trị và quản lý người nhiễm COVID-19 có khả năng gây dịch trong các cơ sở KBCB:
- Thành lập Ban chỉ đạo phòng chống dịch.
- Xây dựng quy trình tiếp nhận và xử lý cụ thể, chi tiết về sàng lọc, phát hiện và cách ly người nhiễm hoặc nghi ngờ nhiễm COVID-19 ngay từ khu vực phòng khám đến khu vực cách ly.
- Tất cả NVYT phải được tập huấn về triệu chứng lâm sàng, điều trị, phương thức lây truyền và quy trình cách ly phòng ngừa trong bệnh viện.
- Có đủ phương tiện bảo đảm cách ly nghiêm ngặt.
- Kiểm tra, đánh giá tính sẵn sàng ngay cả khi chưa có/có dịch.
HƯỚNG DẪN XÂY DỰNG KHU CÁCH LY TRONG CƠ SỞ KHÁM BỆNH, CHỮA BỆNH
COVID-19 là bệnh có khả năng lây nhiễm rất cao. Việc cách ly sớm NB nhiễm hoặc nghi ngờ nhiễm COVID-19 là rất quan trọng. Để thực hiện tốt biện pháp cách ly, các cơ sở KBCB cần luôn có sẵn khu vực và phòng cách ly với đầy đủ phương tiện, NVYT được huấn luyện tuân thủ thực hành các quy trình kỹ thuật khi cách ly:
- Các cơ sở KBCB cần thiết lập khu cách ly ngay tại nơi đón tiếp NB, bao gồm các khu vực chờ khám đối với người nghi ngờ nhiễm COVID-19, khu vực phân loại, buồng cách ly và các phương tiện PHCN, phục vụ quá trình điều trị và chăm sóc NB để thu dung người bệnh COVID-19.
- Các khoa Khám bệnh, khoa cấp cứu, khoa Nhi, khoa Truyền nhiễm bố trí sẵn một buồng cách ly với đầy đủ phương tiện cần thiết để kịp thời cách ly NB khi cần.
1. Mô hình khu cách ly
1.1. Mục đích
- Hạn chế và kiểm soát lây truyền COVID-19 trong môi trường cơ sở KBCB và cho cộng đồng, nhất là NVYT, NB, người nhà NB và khách thăm.
- Cô lập mầm bệnh trong khu vực cách ly để xử lý.
1.2. Nguyên tắc xây dựng khu cách ly
- Nằm ở cuối hành lang, nơi ít người qua lại, cuối hướng gió chính.
- Không để người nhà tham gia chăm sóc, hạn chế tối đa khách thăm.
- Khu cách ly cần được chia thành 3 vùng khác nhau theo nguy cơ lây nhiễm:
+ Vùng có nguy cơ lây nhiễm thấp: Khu vực hành chính, nơi làm việc của NVYT. Khu vực này để biển báo màu xanh và hạn chế người qua lại. NVYT cần mang khẩu trang y tế.
+ Vùng có nguy cơ lây nhiễm trung bình: Khu vực hành lang, buồng đệm để phương tiện chăm sóc và điều trị NB. Khu vực này để biển báo màu vàng. Chỉ có NVYT vào buồng cách ly mới được có mặt ở khu vực này và phải mang phương tiện PHCN đầy đủ, phù hợp với tình huống tiếp xúc.
+ Vùng có nguy cơ lây nhiễm cao: Buồng tiếp nhận, cấp cứu, điều trị người bệnh, nhà vệ sinh, buồng xử lý dụng cụ. Khu vực này để biển báo màu đỏ. NVYT phải mang tối đa phương tiện PHCN và thực hiện VST sau mỗi khi tiếp xúc với. NB, với bề mặt môi trường và trước khi ra khỏi khu vực cách ly.
1.3. Yêu cầu khu vực cách ly
1.3.1. Thiết kế khu cách ly áp dụng cho bệnh viện tuyến tỉnh, thành phố
- Các buồng chức năng:
1) Buồng hành chính.
2) Buồng tiếp nhận NB.
3) Buồng điều trị NB.
4) Buồng NB nhiễm COVID-19 nặng cấp cứu (có đủ phương tiện cấp cứu, điều trị dùng riêng cho từng NB).
5) Buồng lưu NB nghi ngờ nhiễm COVID-19.
6) Buồng xử lý dụng cụ có đủ phương tiện cho khử khuẩn ban đầu: như bồn rửa dụng cụ, tủ sấy khô và hoá chất khử khuẩn.
7) Buồng để vật dụng thiết yếu cho chăm sóc và điều trị NB.
8) Buồng vệ sinh cho người bệnh có đủ bồn rửa tay, khăn lau tay sạch dùng 1 lần và xà phòng rửa tay.
9) Nhà tắm cho NVYT có xà phòng rửa tay.
Các buồng trong khu cách ly đều phải có bồn rửa tay, khăn lau tay, dung dịch VST chứa cồn, xà phòng rửa tay. Bố trí đường di chuyển đi từ vùng có nguy cơ thấp đến vùng có nguy cơ cao.
10) Hệ thống thông khí: Tốt nhất là hệ thống khí áp lực âm tại các buồng cách ly. Trong trường hợp không có hệ thống thông khí áp lực âm, cần tạo luông khí cưỡng bức đi từ khu vực ít nguy cơ nhất đến khu vực có nguy cơ cao nhất (từ vùng xanh tới vùng đỏ). Tần suất trao đổi khí tối thiểu 12 lần/giờ. Khí thoát ra từ khu cách ly cần được khử khuẩn bằng UVC hoặc kết hợp khử khuẩn và lọc HEPA. Nếu không có, khí thoát ra phải đưa vào môi trường trống, không người qua lại.
11) Sàn nhà và tường (chiều cao từ sàn tối thiểu 2 m) cần ốp gạch men, dễ vệ sinh và khử khuẩn.
12) Góc tường nhà và sàn nhà nên thiết kế góc tù hoặc bo tròn, tránh góc cạnh để dễ vệ sinh, không đọng bẩn.
13) Cửa sổ làm bằng vật liệu dễ vệ sinh (kính, ít chi tiết, dễ lau rửa).
1.3.2. Thiết kế buồng cách ly cho bệnh viện tuyến quận, huyện
1) Các bệnh viện trong vùng có nguy cơ xảy ra dịch cần luôn dành một khu vực tại khoa lây hoặc một khu vực riêng biệt trong nội viện để tiếp nhận NB nhiễm hoặc nghi ngờ nhiễm COVID-19.
2) Buồng cách ly cũng phải bố trí sao cho không gần nơi NB khác nằm, nơi nhiều người qua lại.
3) Khu cách ly có thể không có đầy đủ các buồng chức năng như các bệnh viện tuyến trên nhưng tối thiểu phải có các buồng sau:
+ Buồng khám, tiếp nhận NB.
+ Buồng cách ly điều trị NB nặng.
+ Buồng vệ sinh, xử lý dụng cụ (có thể nằm ngay trong buồng cách ly).
4. Khu cách ly cần có hệ thống thông khí cơ học hướng từ buồng cách ly ra vùng ít người qua lại, có cửa sổ thông thoáng với môi trường bên ngoài.
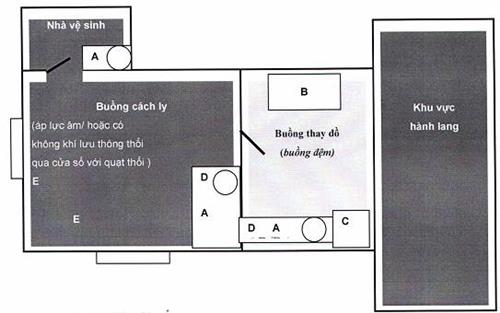
A: Nơi khử khuẩn
B: Tủ đựng PTPHCN, đồ vải và dụng cụ sạch
C: Túi đựng phương tiện PHCN sau sử dụng, chất thải, đồ vải bẩn
D: Bồn rửa tay có xà phòng, dung dịch khử khuẩn tay chứa cồn
E: Cửa sổ mở ra ngoài, xa khu vực dân cư, không người qua lại
Hình 2. Sơ đồ buồng cách ly người nhiễm COVID-19
1.4. Sắp xếp giường bệnh trong buồng cách ly
Nếu có điều kiện, tốt nhất là bố trí mỗi người nhiễm COVID-19 vào một buồng cách ly riêng.
Nếu không có điều kiện hoặc khi có quá nhiều người nhiễm hoặc nghi ngờ nhiễm COVID-19 nhập viện thì bố trí NB nghi ngờ nhiễm vào cùng phòng (cách ly theo nhóm), NB xác định nhiễm COVID-19 vào cùng phòng. Người nghi ngờ nhiễm, chờ kết quả xét nghiệm một phòng. Khoảng cách giữa các giường tối thiểu là 2 mét để dự phòng lây truyền qua đường giọt bắn.
2. Danh mục các dụng cụ cần thiết cần có tại khu/buồng cách ly:
- Các phương tiện cần phải luôn có trong khu cách ly, buồng cách ly, được đó trên xe hoặc tủ tại buồng tiền phòng ngay trước buồng cách ly.
- Các khoa phòng, đơn vị có liên quan (như vệ sinh môi trường, xử lý chất thải, vận chuyển NB...) đến chăm sóc và điều trị người nhiễm hoặc nghi ngờ nhiễm COVID-19 cần phải mang đầy đủ phương tiện PHCN phù hợp với các hoạt động (ủng cao su, tạp dề, khẩu trang, kính...).
- Danh mục các dụng cụ, phương tiện PHCN phải luôn có sẵn ngay tại khu vực cách ly và phải được kiểm tra, bổ sung đủ hàng ngày. Lưu ý có đủ kích cỡ cho người sử dụng và cơ số tối thiểu phải có luôn sẵn sàng (xem Bảng 1).
Bảng 1. Phương tiện, dụng cụ cần luôn có sẵn tại khu/buồng cách ly (Tối thiểu hàng ngày khi có NB năm theo dõi và điều trị)
|
TT |
Dụng cụ |
Cơ số |
|
|
Phương tiện PHCN |
|
|
1 |
Găng tay sạch các cỡ |
150 |
|
2 |
Bộ trang phục phòng hộ |
30 |
|
3 |
Kính mắt, tấm che mặt |
30 |
|
4 |
Mũ che đầu |
50 |
|
5 |
Bốt hoặc bao giày |
30 |
|
6 |
Khẩu trang N95 |
20 |
|
7 |
Khẩu trang y tế |
50 |
|
|
Dụng cụ cần thiết khác |
|
|
1 |
Quần áo NB |
05 |
|
2 |
Vải trải giường |
05 |
|
3 |
Khăn lau tay dùng một lần hoặc khăn giấy |
30 |
|
4 |
Thùng đựng khan |
01 |
|
5 |
Xà phòng rửa tay và dung dịch VST chứa cồn |
05 |
|
6 |
Giá để xà phòng và dung dịch VST chứa cồn |
|
|
7 |
Găng tay vệ sinh |
10 |
|
8 |
Khăn lau bề mặt và giấy thấm lau dịch vương vãi |
05 |
|
9 |
Túi/thùng đựng chất thải các loại có in biểu tượng loại chất thải lây nhiễm |
10/01 |
|
10 |
Túi đựng đồ vải bẩn |
05 |
|
11 |
Thùng đựng đồ vải bẩn có nắp |
01 |
|
12 |
Thùng đựng dụng cụ bẩn |
01 |
|
13 |
Hóa chất khử khuẩn ban đầu và vệ sinh |
|
3. Thông khí
Tăng cường thông khí là biện pháp quan trọng trong phòng ngừa lây nhiễm COVID-19. Có 3 hình thức tăng thông khí:
3.1. Thông khí cơ học:
Tạo phòng thông khí áp lực âm qua việc đưa khí sạch vào phòng và hút khí ô nhiễm ra sao cho tạo được ít nhất 12 lần trao đổi khí mỗi giờ (ACH) và áp lực âm tối thiểu -3Pa. Khí thoát ra được đưa qua hệ thống lọc thô và lọc HEPA kết hợp với khử khuẩn bằng UVC.
3.2. Thông khí tự nhiên:
Không khí vào và ra khỏi phòng hoặc khu vực cách ly qua cửa chính hoặc cửa sổ. Buồng bệnh có 2 cửa sổ đối diện nhau, mở toàn bộ 2 cửa sổ sẽ đảm bảo thông khí trong buồng bệnh tối thiểu 12 ACH. Buồng bệnh khi sử dụng thông khí tự nhiên nên ở cuối chiều gió, có cửa sổ đối lưu 2 chiêu, cửa sổ mở hướng ra khu vực không có người qua lại.
3.3. Thông khí hỗn hợp:
Áp dụng thông khí tự nhiên kết hợp với dùng hệ thống quạt thải khí ra ngoài. Không thải khí ra nơi có nhiều người qua lại, vào hành lang hoặc các phòng khác. Khí thoát ra từ các quạt hút cần được khử khuẩn bằng UVC hoặc kết hợp khử khuẩn và lọc HEPA. Nếu không có, lưu ý chọn vị trí quạt hút sao cho khí thoát ta môi trường trống, không có người qua lại.
Cần tính toán công suất, số quạt hút và thải theo thể tích của buồng để đảm bảo thông khí ít nhất 12 ACH.
SỬ DỤNG PHƯƠNG TIỆN PHÒNG HỘ CÁ NHÂN
Phương tiện PHCN là phương tiện thiết yếu để bảo vệ NVYT trước nguy cơ lây nhiễm khi tiếp xúc với máu, dịch tiết và giọt hô hấp mang các tác nhân gây bệnh truyền nhiễm khi tiếp xúc gần với NB. Phương tiện PHCN cũng được sử dụng để bảo vệ NB không bị nhiễm các vi sinh vật thường trú và vãng lai từ NVYT và môi trường trong bệnh viện. Việc mang phương tiện PHCN khi chăm sóc người nhiễm hoặc nghi nhiễm COVID-19 là biện pháp quan trọng nhất trong phòng ngừa lây nhiễm cho NVYT.
1. Mục đích
Ngăn ngừa nguy cơ lây nhiễm COVID-19 từ NB sang NVYT, NB khác, khách thăm và phát tán ra môi trường xung quanh NB và cộng đồng.
2. Phạm vi áp dụng
Tất cả NVYT, người nhà NB, khách thăm, những người có tiếp xúc với người hoặc mẫu bệnh phẩm từ người nhiễm hoặc nghi ngờ nhiễm COVID-19
3. Nguyên tắc thực hiện
3.1. Nguyên tắc chung
- Sử dụng các phương tiện PHCN theo khuyến cáo của phòng ngừa chuẩn kết hợp với phòng ngừa theo đường lây truyền phù hợp với tình huống trong chăm sóc người nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Đảm bảo luôn sẵn có cơ số phương tiện PHCN tại các khu vực cách ly, buồng đệm của phòng cách ly, phòng XN, khu vực xử lý rác thải, xử lý thi hài.
- Phương tiện PHCN chỉ hiệu quả khi được áp dụng cùng với những biện pháp kiểm soát nhiễm khuẩn khác như tổ chức quy trình sàng lọc, cách ly, vệ sinh môi trường bề mặt, quản lý chất thải.
- Cần tuân thủ đúng chỉ định và quy trình mặc và tháo bỏ phương tiện PHCN.
3.2. Nguyên tắc sử dụng phương tiện phòng hộ cá nhân
1. Luôn mang phương tiện PHCN khi tiếp xúc, thăm khám, chăm sóc cho người nhiễm hoặc nghi ngờ nhiễm COVID-19.
2. Thực hành mặc vào và tháo bỏ phương tiện PHCN phải được thực hiện thuần thục trước khi chăm sóc người nhiễm hoặc nghi ngờ nhiễm COVID-19 và phải được giám sát bởi thành viên đã được đào tạo.
3. Chuẩn bị đầy đủ phương tiện PHCN phù hợp với tình huống sắp thực hiện.
4. Mặc và tháo bỏ phương tiện PHCN trong buồng đệm trước khi vào và sau khi ra khỏi buồng cách ly. Tránh tiếp xúc hoặc điều chỉnh phương tiện PHCN trong buồng cách ly.
5. Phải đảm bảo phương tiện PHCN phủ kín toàn bộ cơ thể.
6. Thay găng khi chuyển từ NB này sang chăm sóc NB khác, thay găng nếu bị rách, VST trước khi mang găng mới.
7. Khi tháo phương tiện PHCN cần chú ý các nguyên tắc sau:
- Mặt ngoài phương tiện PHCN có mức độ nguy cơ nhiễm bẩn cao, khi tháo phải cuộn mặt ngoài vào trong, không được giữ phương tiện PHCN khi tháo.
- Mặt trước của phương tiện PHCN có nguy cơ lây nhiễm cao hơn mặt sau. Tránh đụng chạm tay vào mặt trước của phương tiện PHCN.
8. Phương tiện PHCN chỉ dùng một lần, là chất thải lây nhiễm, sau khi tháo phải bỏ ngay vào thùng chất thải lây nhiễm (thùng màu vàng). Thùng đựng chất thải phải đủ lớn và phải có nắp đậy tự động.
4. Các loại phương tiện phòng hộ cá nhân
4.1. Loại phương tiện phòng hộ cá nhân
Trên thực tế hiện nay có nhiều kiểu loại phương tiện PHCN, có thể xếp vào 2 loại sau:
Loại thứ nhất: Loại quần, áo choàng và mũ trùm đầu riêng biệt:
- Áo choàng chống thấm hoặc áo choàng có kèm tấm choàng chống thấm.
- Quần chống thấm.
- Tạp dề chống thấm.
- Khẩu trang y tế.
- Khẩu trang hiệu lực lọc cao (ví dụ N95).
- Kính bảo hộ hoặc tấm che mặt.
- Găng tay y tế.
- Mũ chụp tóc (loại trùm kín đầu và cổ).
- Bao giầy loại ống cao.
- Ủng cao su.
Loại 2: Loại quần liền, áo choàng và mũ trùm đầu:
- Bộ quần, áo choàng, mũ.
- Bao giầy loại ống cao.
- Tạp dề chống thấm.
- Khẩu trang y tế.
- Khẩu trang N95.
- Kính bảo hộ hoặc tấm che mặt.
- Găng tay y tế.
- Găng cao su.
- Bao giầy chống thấm loại ống cao.
- Ủng cao su.
4.2. Một số tiêu chí kỹ thuật
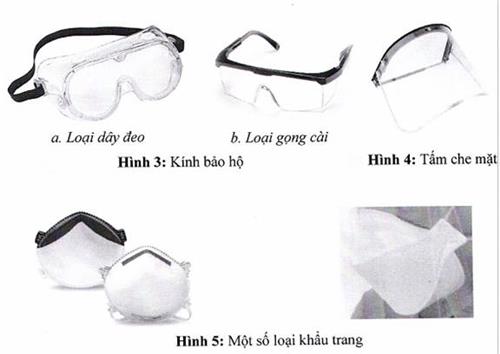
- Kính bảo hộ và tấm che mặt phải bó sát vào khuôn mặt và ngăn chặn không để dịch thấm vào (Hình 3 và Hình 4).
- Khẩu trang y tế đạt tiêu chuẩn, không thấm nước, có thanh kim loại giúp uốn khít sống mũi, ngăn chặn không khí, dịch bắn đi qua.
- Khẩu trang có hiệu lực lọc cao (ví dụ khẩu trang đạt tiêu chuẩn N95 hoặc FFP2 hoặc tương đương).
- Găng tay: Khuyến cáo dùng găng làm bằng chất liệu nitrile hơn chất liệu latex, với kích thước phù hợp với tay của người sử dụng.
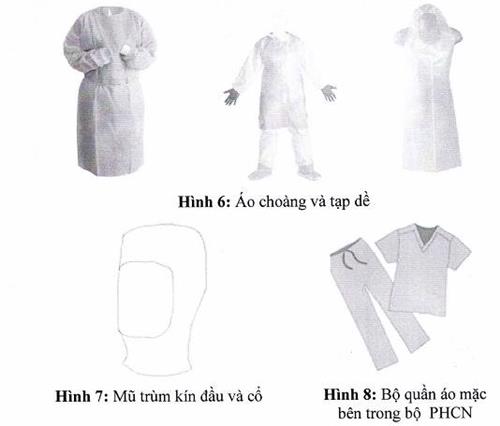
- Áo choàng có chiều dài đến giữa đùi, tay dài và cổ tay bo và tạp dề phải bằng chất liệu không thấm máu và dịch.
- Ủng cao su không thủng rách, kích cỡ phù hợp với chân của người sử dụng.
- Bao giầy cao đến gần gối, bằng chất liệu không thấm nước và, chống trượt.
- Mũ che đầu và cổ, có chỗ mở phía trước để tháo ra sau.
- Bộ quần áo mặc bên trong trước khi mang trang PHCN.
5. Quy trình mang và tháo bỏ phương tiện phòng hộ cá nhân
5.1. Mang và tháo khẩu trang
5.1.1. Khẩu trang y tế:
* Kỹ thuật mang khẩu trang:
- Vệ sinh tay.
- Mở bao gói, lấy khẩu trang ra khỏi bao, một tay cầm vào 1 cạnh bên.
- Đặt khẩu trang lên mặt, mặt chống thấm (màu xanh) quay ra ngoài, mặt thấm hút (màu trắng) quay vào trong. 1 tay giữ mặt trước khẩu trang cố định trên mặt, 1 tay luồn 1 bên dây đeo qua tai sau đó làm ngược lại với bên kia.
- Dùng ngón 2 đầu ngón tay trỏ ấn chỉnh thanh kim loại trên mũi sao cho ôm sát sống mũi và mặt.
- 2 ngón tay cầm mép dưới của khẩu trang kéo nhẹ xuống dưới, đưa vào trong để khẩu trang bám sát vào mặt dưới cằm.
* Kỹ thuật tháo khẩu trang:
- Tháo dây đeo khẩu trang, tay không chạm vào khẩu trang, loại bỏ khẩu trang vào thùng thu gom chất thải theo đúng quy định.
- Vệ sinh tay.
5.1.2. Khẩu trang có hiệu lực lọc cao (ví dụ khẩu trang N95)
* Kỹ thuật mang khẩu trang:
- Vệ sinh tay.
- Mở bao gói, đặt khẩu trang vào lòng bàn tay, cạnh có kim loại ôm vào sống mũi, hướng ra trước, để dây đeo thả tự do dưới bàn tay.
- Đặt khẩu trang phía dưới cằm, phần che mũi hướng lên trên.
- Kéo dây trên qua đầu và đặt vào vùng chẩm, dây trên tai. Kéo dây dưới qua đầu và đặt vào sau gáy, dưới tai. Lưu ý không để hai dây bắt chéo nhau ở sau đầu.
- Kiểm tra và chỉnh lại dây đeo nếu bị xoắn, vặn.
- Đặt đầu ngón tay trỏ của 2 tay tại đỉnh sống mũi, ấn chỉnh phần che mũi sao cho khẩu trang ôm khít mũi.
- Kiểm tra độ kín của khẩu trang:
+ Thử nghiệm hít vào (âm tính): thở ra từ từ, nếu khẩu trang kín, áp lực âm làm cho khẩu trang bám sát vào khuôn mặt. Nếu khẩu trang không kín, không khí sẽ qua lỗ hở đi vào khẩu trang, cần điều chỉnh lại độ căng của dây đeo và làm lại thử nghiệm hít vào.
+ Thử nghiệm thở ra (dương tính): thở ra mạnh, nếu khẩu trang kín, áp lực dương tạo luồng không khí bên trong khẩu trang. Nếu khẩu trang không kín, cân điều chỉnh lại độ căng của dây đeo và làm lại thử nghiệm thở ra.
* Kỹ thuật tháo khẩu trang:
- Tháo dây dưới bằng cách cầm vào phần dây sau đầu, sau đó tháo dây trên qua đầu, không để tay chạm vào khẩu trang khi tháo.
- Vệ sinh tay.
5.1.3. Những lưu ý khi mang và tháo khẩu trang
- Đeo khẩu trang đúng chiều trên, dưới.
- Đeo khẩu trang đúng mặt trong, ngoài.
- Không chạm tay vào mặt trong khẩu trang khi đeo.
- Đặt khẩu trang cẩn thận để che kín miệng và mũi.
- Chỉnh gọng mũi và dây đeo để đảm bảo khẩu trang ôm sát sống mũi va khuôn mặt.
- Tay không chạm vào mặt trước khẩu trang khi loại bỏ khẩu trang.
- Sau khi loại bỏ hoặc bất cứ khi nào vô tình chạm vào khẩu trang đã sử dụng, cần làm sạch tay bằng dung dịch VST có chứa cồn hoặc rửa tay bằng xà phòng và nước.
- Thay khẩu trang sau mỗi khi thực hiện thủ thuật sạch/vô khuẩn, ngay khi thấy khẩu trang bị nhiễm bẩn hoặc bị ẩm/ướt hoặc sau mỗi ca làm việc.
- Không sử dụng lại khẩu trang đã qua sử dụng.
5.2. Trình tự mang phương tiện phòng hộ cá nhân
Bước 1: Vệ sinh tay.
Bước 2: Đi bốt/bao giầy.
Bước 3: Mặc quần và áo choàng (mang tạp dề nếu có chỉ định).
Bước 4: Mang khẩu trang.
Bước 5: Mang kính bảo hộ (đối với loại có gọng cài tai).
Bước 6: Đội mũ trùm kín tóc, đầu, tai, dây đeo khẩu trang.
Bước 7: Mang tấm che mặt hoặc kính bảo hộ (nếu là loại dây đeo ngoài mũ).
Bước 8: Mang găng sạch.
5.3. Trình tự tháo bỏ phương tiện phòng hộ cá nhân
5.3.1. Loại quần, áo choàng và mũ trùm đầu rời
Bước 1: Tháo găng. Khi tháo cuộn mặt trong găng ra ngoài, bỏ vào thùng đựng chất thải. Nếu có mang tạp dề, tháo tạp dề, cởi dây dưới trước, dây trên sau, cuộn ngược mặt trong của tạp dề ra ngoài, bỏ vào thùng chất thải.
Bước 2: Vệ sinh tay.
Bước 3: Tháo bỏ áo choàng, cuộn mặt trong của áo choàng ra ngoài và bỏ vào thùng chất thải.
Bước 4: Vệ sinh tay.
Bước 5: Tháo bỏ quần và ủng hoặc bao giầy cùng lúc, lộn mặt trong của quần ra ngoài, bỏ vào thùng chất thải. Nếu mang ủng, đặt ủng vào thùng có dung dịch khử khuẩn.
Bước 6: Vệ sinh tay.
Bước 7: Tháo kính bảo hộ hoặc tấm che mặt.
Bước 8: Vệ sinh tay.
Bước 9: Tháo bỏ mũ trùm bằng cách luồn tay vào mặt trong mũ.
Bước 10: Tháo khẩu trang (cầm vào phần dây đeo phía sau đầu hoặc sau tai).
Bước 11: Vệ sinh tay.
5.3.2. Loại bộ phòng hộ quần liền áo và mũ
Bước 1: Tháo găng. Khi tháo cuộn mặt trong găng ra ngoài, bỏ vào thùng đựng chất thải. Nếu có mang tạp dề, tháo tạp dề, cởi dây dưới trước, dây trên sau, cuộn ngược mặt trong của tạp dề ra ngoài, bỏ vào thùng chất thải;
Bước 2: Vệ sinh tay.
Bước 3: Tháo kính bảo hộ hoặc tấm che mặt.
Bước 4: Vệ sinh tay.
Bước 5: Tháo bỏ mũ, áo, quần. Khi tháo để mặt trong của trang phục lộn ra ngoài và loại bỏ vào thùng gom chất thải.
Bước 6: Vệ sinh tay.
Bước 7: Tháo ủng hoặc bao giầy, lộn mặt trong ra ngoài và bỏ vào thùng chất thải. Nếu mang ủng, đặt ủng vào thùng có dung dịch khử khuẩn.
Bước 8: Vệ sinh tay.
Bước 19: Tháo khẩu trang (cầm vào phần dây đeo phía sau đầu hoặc sau tai).
Bước 10: Vệ sinh tay.
Chú ý: Tháo bỏ trang phục PHCN tại buồng đệm của khu, phòng cách ly.
6. Kiểm tra, giám sát việc sử dụng phương tiện phòng hộ cá nhân
- Khoa KSNK và phòng Điều dưỡng: chịu trách nhiệm kiểm tra, giám sát, huấn luyện việc sử dụng phương tiện PHCN của NVYT.
- Nội dung giám sát:
+ Luôn có sẵn phương tiện PHCN tại buồng đệm của khu, phòng cách ly.
+ Nhân viên y tế sử dụng đủ và đúng phương tiện PHCN cần thiết.
+ Phân loại, thu gom, xử lý phương tiện PHCN đã qua sử dụng.
- Phương pháp giám sát: bằng quan sát trực tiếp và ghi phiếu giám sát.
VỆ SINH TAY
Vệ sinh tay là một trong những biện pháp quan trọng giúp phòng ngừa và kiểm soát lây nhiễm COVID-19. Việc VST cần phải được thực hiện thường xuyên tất cả lúc, tất cả nơi theo đúng 5 thời điểm VST trong quá trình chăm sóc và điều trị NB.
Tất cả các cơ sở KBCB cần phải:
1. Trang bị phương tiện vệ sinh tay
Tăng cường bổ sung đầy đủ phương tiện VST tại tất cả các khu vực có người nhiễm hoặc nghi ngờ nhiễm COVID-19.
1.1. Phương tiện vệ sinh tay với xà phòng và nước sạch
- Các bồn VST phải được bố trí trong buồng cách ly, buồng đệm, buồng hành chính, nơi pha chế dịch, thuốc, buồng xét nghiệm, buồng dinh dưỡng, nơi xử lý chất thải, đồ vải bẩn, nhà đại thể thuận tiện cho NB và NVYT sử dụng.
- Các bồn VST có đầy đủ dung dịch xà phòng, nước sạch, thùng đựng khăn lau tay (bằng vải hoặc giấy) dùng một lần.
Một số quy định cụ thể:
- Bồn VST phải đủ sâu để tránh nước bắn ra bên ngoài và bắn vào người rửa, không có góc cạnh, bề mặt nhẵn, không có vết cáu bẩn và ứ đọng nước. Chiều cao của bồn phù hợp với chiều cao của người VST.
- Vòi nước: gắn cố định vào trong tường. Khóa vòi nên sử dụng loại tự động, đạp chân hoặc có cần gạt.
- Hệ thống nước: nước máy, đường dẫn nước nên đặt chìm vào trong tường, nhưng phải dễ cho lắp đặt, vệ sinh, khử khuẩn khi cần thiết.
- Xà phòng và giá để xà phòng VST: tốt nhất là xà phòng dạng dung dịch, chứa trong bình kín, có bơm định lượng chuẩn, lắp đặt phù hợp. Nếu dùng xà phòng bánh thì cần để trong hộp có nắp đậy kín, để nơi khô ráo, tránh nước bắn.
- Khăn lau tay sử dụng một lần: có thể bằng giấy dùng một lần hoặc khăn sợi bông tái sử dụng để trong hộp cấp khăn, kín, dễ lấy khăn ra.
- Thùng đựng khăn bẩn: thiết kế sao cho thao tác bỏ khăn vào thùng được dễ dàng, không phải đụng chạm tay vào nắp.

Hình 9: Rửa tay dưới vòi nước chảy
1.2. Phương tiện vệ sinh tay có chứa còn/cồn trong chlorhexidin
- Trang bị lọ (chai) dung dịch khử khuẩn tay có chứa cồn có nồng độ từ 60% - 80% hoặc cồn trong chlorhexidin ở tất cả những khu vực chăm sóc NB, mỗi đầu giường NB nặng, NB cấp cứu. Trên các xe tiêm, xe thay băng, bàn khám bệnh. Trên tường ngay cạnh lối (cửa) vào buồng bệnh, phòng đệm, phòng cách ly, trước cửa thang máy, hành lang... nơi có nguy có phơi nhiễm với máu, dịch cơ thể NB.
- Cần phải thường xuyên thay và vệ sinh các bình chứa dung dịch cồn khử khuẩn tay và đảm bảo bình luôn sẵn có tại những vị trí đã quy định.
- Chai đựng dung dịch cồn VST, có bơm định chuẩn, có giá gắn cố định vào tường hoặc treo các đầu giường NB, trước cửa buồng bệnh, xe tiêm...
2. Chỉ định vệ sinh tay
2.1. Vệ sinh tay với xà phòng và nước sạch
- Bất cứ khi nào bàn tay có dính máu và dịch cơ thể có thể nhìn thấy được bằng mắt, trong quá trình chăm sóc, điều trị NB (làm thủ thuật xâm lấn, chăm sóc vệ sinh thân thể NB, xử lý dụng cụ bẩn, chất thải,...) mặc dù có mang găng tay và nghi ngờ thủng găng hoặc tháo bất cẩn làm tiếp xúc với nguồn nhiễm.
- Vệ sinh tay bằng xà phòng và nước cũng cần được thực hiện trước và sau buổi làm việc, sau khi đi vệ sinh, sau thu gom đồ vải, dụng cụ, chất thải...
2.2. Vệ sinh tay với dung dịch có chứa cồn
- Chỉ VST với dung dịch có chứa cồn khi bàn tay khô, không dính máu và dịch cơ thể có thể nhìn thấy được bằng mắt, trong chăm sóc, điều trị, sau khi tháo bỏ phương tiện PHCN.
- Tại những nơi không thể lắp đặt bồn rửa tay và những nơi các thao tác chăm sóc không có nguy cơ dính máu và dịch cơ thể NB bằng mắt thường có thể phát hiện được.
- Chỉ định VST với dung dịch có chứa cồn: tương tự như trong VST với xà phòng và nước nếu không có dính máu và dịch cơ thể có thể nhìn thấy.
- Thời điểm NVYT cần VST: 5 thời điểm bắt buộc NVYT phải tuân thủ nghiêm ngặt VST (theo khuyến cáo của Tổ chức Y tế Thế giới).
|
1. Trước khi tiếp xúc với NB |
|
|
2. Trước khi làm thủ thuật vô trùng |
|
|
3. Sau khi tiếp xúc với máu và dịch cơ thể |
|
|
4. Sau khi tiếp xúc NB |
|
|
5. Sau khi đụng chạm vào những vùng xung quanh NB |
Hình 10. Các thời điểm VST khi chăm sóc người bệnh
+ Ngoài ra cần phải VST trong một số trường hợp sau:
• Trong quy trình mặc và tháo phương tiện PHCN.
• Trước khi mang găng tay.
• Khi chuyển chăm sóc từ nơi nhiễm sang nơi sạch trên cùng NB.
• Trước khi kết thúc công việc tại khu vực cách ly đi ra bên ngoài.
• Trước khi trở về gia đình.
3. Kỹ thuật
3.1. Vệ sinh tay bằng xà phòng và nước (Hình 11)
- Bước 1: Làm ướt hai lòng bàn tay bằng nước. Lấy xà phòng và chà hai lòng bàn tay vào nhau cho sủi bọt.
- Bước 2: Chà lòng bàn tay này lên mu và kẽ ngoài các ngón tay bàn tay kia và ngược lại.
- Bước 3: Chà hai lòng bàn tay vào nhau, miết mạnh các kẽ trong ngón tay.
- Bước 4: Chà mặt ngoài các ngón tay của bàn tay này vào lòng bàn tay kia.
- Bước 5: Dùng bàn tay này xoay ngón cái của bàn tay kia và ngược lại.
- Bước 6: Xoay các đầu ngón tay này vào lòng bàn tay kia và ngược lại. Rửa sạch tay dưới vòi nước chảy.
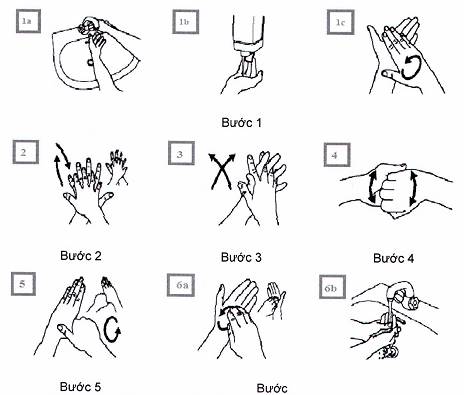
Hình 11: Kỹ thuật VST với xà phòng và nước sạch
3.2. Vệ sinh tay với dung dịch có chứa cồn (Hình 12)
- Bước 1: Lấy 3ml - 5ml dung dịch VST có chứa cồn/cồn trong chlorhexidin và chà hai lòng bàn tay vào nhau.
- Bước 2: Chà lòng bàn tay này lên mu và kẽ ngoài các ngón tay của bàn tay kia và ngược lại.
- Bước 3: Chà hai lòng bàn tay vào nhau, miết mạnh các kẽ trong ngón tay.
- Bước 4: Chà mặt ngoài các ngón tay của bàn tay này vào lòng bàn tay kia.
- Bước 5: Dùng bàn tay này xoay ngón cái của bàn tay kia và ngược lại.
- Bước 6: Xoay các đầu ngón tay này vào lòng bàn tay kia và ngược lại cho đến khi bàn tay khô.
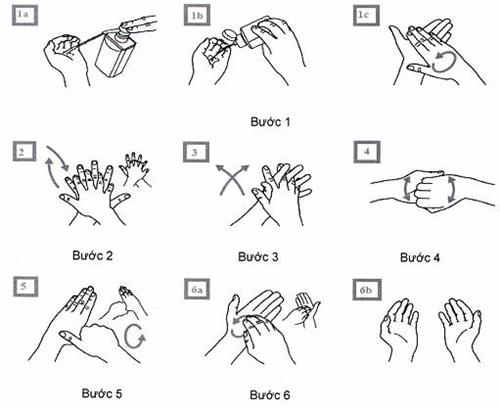
Hình 12: Kỹ thuật VST với dung dịch có chứa cồn (20 giây-30 giây)
Ghi chú:
- Cắt ngắn móng tay.
- Tháo bỏ toàn bộ trang sức trên bàn tay (nhẫn, vòng đeo tay, đồng hồ...).
- Kỹ thuật tương tự như VST với xà phòng và nước. Mỗi bước chà tối thiểu 5 lần.
Xem thêm Hướng dẫn thực hành vệ sinh tay trong các cơ sở khám bệnh, chữa bệnh ban hành theo Quyết định số 3916/QĐ-BYT ngày 28/8/2017 của Bộ trưởng Bộ Y tế.
XỬ LÝ DỤNG CỤ
Tất cả các dụng cụ sau khi sử dụng cho chăm sóc và điều trị người nhiễm hoặc nghi ngờ nhiễm COVID-19 đều là những dụng cụ có nguy cơ lây nhiễm, nêu không được xử lý đúng quy trình sẽ có nguy cơ phát tán và lây nhiễm cho NVYT và cộng đồng.
1. Mục đích
- Nhân viên thực hiện xử lý dụng cụ tuân thủ nghiêm ngặt quy trình làm sạch, khử khuẩn và tiệt khuẩn các dụng cụ sau chăm sóc và điều trị NB đúng quy định.
- Bảo đảm an toàn cho NB, NVYT và cộng đồng.
2. Nguyên tắc
- Thiết bị và dụng cụ y tế chuyên dụng khi sử dụng trong chăm sóc và điều trị NB tốt nhất là dùng một lần (ví dụ: như các dụng cụ hỗ trợ hô hấp như ống hút đờm, mask khí dung, dây máy thở, bộ chăm sóc răng miệng...). Dụng cụ tái sử dụng đều phải được xử lý theo đúng quy định của BYT.
- Tất cả các thiết bị và dụng cụ y tế dùng một lần nhưng xử lý dùng lại cần phải được làm sạch, khử khuẩn theo đúng hướng dẫn của nhà sản xuất và quy định của BYT.
- Bảo đảm dụng cụ và thiết bị dùng cho NB được xử lý, khử khuẩn và tiệt khuẩn đúng quy trình, đảm bảo chức năng hoạt động của dụng cụ và luôn được cung cấp đầy đủ, sẵn sàng.
- Bảo đảm có đầy đủ quy trình hướng dẫn khử khuẩn cho tất cả các dụng cụ và phương tiện chăm sóc NB tại nơi phát sinh và nơi xử lý dụng cụ.
- Cung cấp đầy đủ phương tiện, hóa chất, vật tư tiêu hao, phương tiện PHCN cho người xử lý (nhất là kính bảo hộ, tấm che mặt, áo choàng không thấm nước, găng tay cao su dài quá khuỷu tay, ủng cao su).
- Nhân viên làm công tác khử khuẩn, tiệt khuẩn phải được huấn luyện, có chứng chỉ đào tạo về khử khuẩn tiệt khuẩn.
- Việc khử khuẩn, tiệt khuẩn phải được kiểm tra, giám sát chất lượng dụng cụ (test thử, hồ sơ lưu trữ), đảm bảo sự an toàn cho NVYT, môi trường, khi thu gom, vận chuyển và xử lý làm sạch, khử khuẩn.
- Thống kê, báo cáo việc xử lý, cung cấp các dụng cụ chăm sóc và điều trị người nhiễm hoặc nghi ngờ nhiễm COVID-19.
3. Đối tượng và phạm vi áp dụng
3.1. Đối tượng áp dụng
- Nhân viên xử lý dụng cụ (tại khu vực cách ly, đơn vị lâm sàng, cận lâm sàng liên quan tới chăm sóc người nhiễm hoặc nghi ngờ nhiễm COVID-19 và đơn vị tiệt khuẩn trung tâm).
- Nhân viên y tế trực tiếp chăm sóc tại các đơn vị chăm sóc điều trị người nhiễm hoặc nghi ngờ nhiễm COVID-19.
3.2. Phạm vi áp dụng
- Khu/phòng cách ly.
- Đơn vị tiệt khuẩn trung tâm/khoa KSNK.
- Khu vực tiếp nhận, phân loại, thăm khám người nhiễm hoặc nghi ngờ nhiễm COVID-19.
4. Phương tiện
4.1. Phương tiện khử khuẩn, tiệt khuẩn
- Phương tiện PHCN: khẩu trang, găng tay cao su và tạp dề chống thấm nước, kính bảo hộ hoặc tấm che mặt, ủng (những vùng có chỉ định).
- Cung cấp đủ nước sạch.
- Thùng ngâm dụng cụ có nắp đậy, có dung tích phù hợp với các loại dụng cụ.
- Bồn rửa dụng cụ (làm bằng vật liệu dễ làm sạch và khử khuẩn).
- Máy rửa dụng cụ.
- Máy tiệt khuẩn hơi nước, tủ sấy khô.
- Máy tiệt khuẩn nhiệt độ thấp (ETO, Plasma...)
4.2. Hoá chất
- Dung dịch làm sạch: các chất tẩy rửa/enzyme, chất khử khuẩn chứa enzyme.
- Dung dịch khử khuẩn mức độ trung bình:
+ Các hợp chất Clo: Sodium hypochloric: Presept, Javel, Chloramin B...
+ Hợp chất có chứa Enzym: Cidexzym...
- Dung dịch khử khuẩn bậc cao: glutaraldehyde ≥ 2%, orthophthaldehyde 0,55%, Peracetic acid...
4.3. Nước: Nước sạch, nước vô khuẩn.
5. Cách thực hiện
5.1. Tại khu vực/buồng cách ly
5.1.1. Chuẩn bị
- Nhân viên xử lý dụng cụ mang đầy đủ phương tiện PHCN (khẩu trang, găng tay cao su và tạp dề chống thấm nước, kính bảo hộ/tâm che mặt) trước khi xử lý dụng cụ.
- Chuẩn bị đủ dụng cụ, phương tiện cho làm sạch, khử khuẩn:
+ Bồn rửa dụng cụ - máy rửa dụng cụ.
+ Hóa chất.
+ Dụng cụ làm sạch (cọ, bàn chải, cây làm sạch ống...).
+ Nước sạch, nước vô khuẩn.
5.1.2. Quy trình thực hiện
Pha hóa chất làm sạch và khử khuẩn theo đúng hướng dẫn
- Dụng cụ ngay sau khi sử dụng cho NB, NVYT phải xử lý ngay:
Ngâm ngập dụng cụ vào dung dịch làm sạch (tẩy rửa) hoặc dung dịch enzym và sau đó ngâm vào dung dịch khử khuẩn mức độ trung bình theo đúng quy định về thời gian, nồng độ dung dịch (xem Phụ lục 4).
+ Xả sạch hoá chất dưới vòi nước sạch. Làm sạch dụng cụ dưới mặt nước.
- Để khô/sấy dụng cụ, cho vào thùng kín có ghi tên dụng cụ người nhiễm hoặc nghi ngờ nhiễm COVID-19 và khi đưa ra ngoài phải bỏ vào trong bao/hộp màu vàng mới chuyển đi.
- Trước khi chuyển phải gọi điện báo có chuyển dụng cụ tới đơn vị tiệt khuẩn trung tâm/khoa KSNK.
5.2. Tại trung tâm tiệt khuẩn, khoa Kiểm soát nhiễm khuẩn
Phải bố trí khu vực tiếp nhận và xử lý ngay các dụng cụ từ khu vực cách ly đưa xuống, ưu tiên làm ngay, xử lý riêng giúp ngăn ngừa phát tán và lây nhiễm trong khu vực và sang khoa khác.
5.2.1. Chuẩn bị phương tiện
- Bố trí phương tiện và người xử lý riêng dụng cụ của người nhiễm hoặc nghi ngờ nhiễm COVID-19 tại khu vực cách ly nếu có thể được.
- Nhân viên xử lý dụng cụ mang đầy đủ phương tiện PHCN trước khi xử lý dụng cụ (gồm: khẩu trang, găng tay cao su và tạp dề chống thấm nước, kính bảo hộ/tấm che mặt).
- Chuẩn bị đủ dụng cụ, phương tiện cho làm sạch, khử khuẩn:
+ Bồn làm sạch dụng cụ - máy làm sạch dụng cụ.
+ Hóa chất.
+ Dụng cụ làm sạch (cọ, bàn chải, cây làm sạch các lòng ống...).
+ Nước sạch, nước tiệt khuẩn.
+ Máy rửa, làm sạch và khử khuẩn dụng cụ đa năng (có thể rửa nhiều loại dụng cụ kim loại và dụng cụ nhựa hỗ trợ đường thở).
+ Máy tiệt khuẩn hơi nước cho dụng cụ chịu nhiệt.
+ Máy tiệt khuẩn nhiệt độ thấp.
5.2.2. Quy trình thực hiện
* Trường hợp làm sạch và khử khuẩn bằng tay (không có máy rửa và khử khuẩn dụng cụ):
- Dụng cụ cần tháo rời được mở các khớp, chỗ nối và cho vào các khay, giá để dụng cụ theo đúng quy định của nhà sản xuất.
- Pha hóa chất khử khuẩn theo đúng hướng dẫn (Phụ lục 4).
- Ngâm ngập ngay dụng cụ vào dung dịch khử khuẩn đã được pha theo đúng nồng độ và thời gian đã quy định.
- Cọ rửa và làm sạch dụng cụ dưới mặt nước của bồn ngâm dụng cụ đánh chải nhẹ tay tránh văng bắn.
- Xả sạch hóa chất dưới vòi nước chảy.
- Làm khô dụng cụ (tủ sấy, lau khô).
- Ngâm, xịt chất bôi trơn để bảo vệ dụng cụ.
- Chuyển các dụng cụ sang khu vực đóng gói (dán nhãn, test kiểm chuẩn, ghi hạn sử dụng) và chuyển tiệt khuẩn.
Làm sạch và khử khuẩn bằng máy chuyên dụng
- Dụng cụ cần tháo rời được mở các khớp, chỗ nối và cho vào các khay, giá để dụng cụ theo đúng quy định của nhà sản xuất.
- Cài đặt chương trình rửa của máy (dụng cụ chịu nhiệt và không chịu nhiệt).
+ Dụng cụ chịu nhiệt: xà phòng, nước, nhiệt độ 90°C.
+ Dụng cụ không chịu nhiệt: xà phòng, nước, nhiệt độ < 50°C.
+ Hóa chất: theo khuyến cáo của nhà sản xuất máy và dụng cụ.
+ Cho dung dịch bôi trơn vào máy.
- Cho máy hoạt động theo chương trình đã cài đặt.
- Kết thúc chu trình, lấy dụng cụ ra khỏi máy đóng gói theo quy định.
- Trong trường hợp máy rửa không có chế độ làm khô: đưa dụng cụ vào máy sấy khô hoặc làm khô bằng lau tay với các tấm vải khô, sạch trước khi đóng gói,
- Tiến hành quy trình tiệt khuẩn.
- Dụng cụ sau tiệt khuẩn phải được lưu trữ trong tủ kín có cửa và phòng lưu trữ thoáng mát (tốt nhất là phòng sạch có máy lạnh duy trì nhiệt độ 20°C-22°C, độ ẩm <60%).
- Phân phát theo yêu cầu hàng ngày của khu vực chăm sóc người nhiễm hoặc nghi ngờ nhiễm COVID-19.
Chú ý:
- Sau khi kết thúc công việc, nhân viên xử lý dụng cụ ở mỗi vùng phải cởi bỏ phương tiện PHCN và VST mới được đi sang khu vực khác.
- Vệ sinh khu vực xử lý dụng cụ mỗi cuối ca/ngày làm việc.
6. Kiểm tra giám sát tuân thủ quy trình làm sạch, khử khuẩn, tiệt khuẩn
Trưởng khoa, điều dưỡng trưởng thường xuyên kiểm tra giám sát việc tuân thủ nghiêm ngặt:
- NVYT có đầy đủ phương tiện, vật tư tiêu hao, hóa chất và phương tiện PHCN khi xử lý dụng cụ.
- Giám sát quy trình là sạch, khử, tiệt khuẩn ngay tại khu vực phát sinh dụng cụ bẩn (phòng khám, cách ly, xét nghiệm..).
- Giám sát quy trình mặc/loại bỏ phương tiện PHCN của NVYT làm việc tại khu vực có liên quan đến những NB này.
- Lưu danh sách NVYT làm việc xử lý dụng cụ, thường xuyên theo dõi và giám sát phát hiện những dấu hiệu lây nhiễm.
Xem thêm Hướng dẫn khử khuẩn, tiệt khuẩn trong các cơ sở khám bệnh, chữa bệnh ban hành theo Quyết định số 3671/QĐ-BYT ngày 27/9/2012 của Bộ trưởng Bộ Y tế.
XỬ LÝ ĐỒ VẢI
1. Mục đích
- Nhân viên y tế tuân thủ đúng quy trình xử lý đồ vải của người nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Bảo đảm an toàn cho người bệnh, NVYT, người nhà người bệnh, khách thăm và cộng đồng.
2. Các nguyên tắc và quy định chung
- Không giũ, đổ, đếm đồ vải thu gom từ quá trình chăm sóc và điều trị người nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Đồ vải sau khi thu gom phải được gói kín, vận chuyển ngay xuống nhà giặt bằng phương tiện riêng và phải được giặt ngay, giặt riêng không ngâm, không lưu đồ vải bẩn.
- Đồ vải của người nhiễm hoặc nghi ngờ nhiễm COVID-19 tại khu vực thăm khám, buồng bệnh, buồng cách ly sau khi sử dụng phải được thu gom vào túi màu vàng có dán hoặc ghi rõ “Đồ vải có nguy cơ chứa COVID-19”.
- Túi đựng đồ vải phải không rách, không thủng và không thấm nước.
- Nhân viên thu gom, vận chuyển và xử lý đồ vải bẩn phải tuân thủ việc mang và tháo bỏ phương tiện phòng hộ theo đúng hướng dẫn. Tuân thủ VST.
- Giặt đồ vải bằng máy với chế độ nhiệt cao và hóa chất. Trong trường hợp không có máy giặt, phải giặt bằng tay đồ vải cần được ngâm hóa chất khử khuẩn trước khi giặt với nồng độ Clo hoạt tính 0,05% (xem Phụ lục 4).
- Giặt, sấy hoặc phơi khô theo đúng quy trình xử lý đồ vải lây nhiễm.
3. Đối tượng và phạm vi áp dụng
3.1. Đối tượng áp dụng
- Nhân viên nhà giặt, nhân viên thu gom vận chuyển đồ vải.
- Nhân viên tại khu cách ly hoặc buồng cách ly, nơi tiếp nhận NB.
3.2. Phạm vi áp dụng
- Buồng bệnh, phòng cách ly.
- Nhà giặt.
- Khu vực khác có liên quan đến đồ vải của người người nhiễm hoặc nghi ngờ nhiễm COVID-19.
4. Phương tiện
- Máy giặt có chế độ giặt nhiệt độ 60°C-70°C, máy sấy khô.
- Túi màu vàng loại không thủng, có dây buộc và ký hiệu đồ vải lây nhiễm nguy cơ cao (đồ vải người bệnh COVID-19), thùng màu vàng, xe chuyên chở đồ vải lây nhiễm riêng.
- Phương tiện PHCN cho nhân viên thu gom, vận chuyển và giặt.
- Hóa chất giặt: Xà phòng, chất tẩy, chất khử khuẩn (Javel, Cloramin B).
5. Thực hiện
5.1. Tại buồng bệnh/buồng cách ly
- Nhân viên thu gom đồ vải bẩn phải mang đầy đủ phương tiện PHCN theo quy định trước khi thực hiện và VST sau khi kết thúc công việc.
- Đồ vải trong phòng bệnh/khu vực cách ly phải được thu gom vào túi màu vàng chống thấm đặt trong thùng có nắp đậy kín và buộc kín trước khi chuyển đến nhà giặt.
- Đồ vải dùng một lần: Áo choàng, mũ, khẩu trang, bao giầy đều được bỏ vào túi màu vàng, và cho vào thùng có nắp đậy và buộc chặt miệng túi khi chuyển xuống nhà lưu giữ chất thải y tế lây nhiễm để thiêu hủy.
- Tất cả túi đựng đồ vải khi chuyển ra ngoài phải cho vào một bao khác rồi chuyển nhà giặt, bao ghi nhãn “Đồ vải có nguy cơ chứa COVID-19”.
- Nhân viên nhà giặt đến lấy theo giờ đã quy định hoặc đột xuất theo yêu cầu.
5.2. Tại nhà giặt
- Đồ vải sau khi thu gom về nhà giặt được cho ngay vào máy giặt ngay và giặt, theo chế độ giặt hóa chất hoặc xà phòng với nhiệt độ 60°C-70°C. Ngâm đồ vải của người nhiễm hoặc nghi ngờ nhiễm COVID-19 đã sử dụng vào dung dịch hóa chất; chứa 0,01%-0,05% Clo hoạt tính tùy mức độ ô nhiễm của đồ vải trong tối thiểu 20 phút trước khi giặt. Với những cơ sở giặt bằng máy giặt thì sử dụng luôn máy giặt để ngâm đồ vải.
- Tốt nhất là sấy khô, nếu không có điều kiện có thể phơi quần áo tại nơi riêng, cao ráo, có nhiều ánh nắng.
- Đồ vải sau khi phơi đem vào phải được là phẳng để vào tủ kín, khô ráo.
Lưu ý: với những nơi không có máy giặt, đồ vải sau khi chuyển đến được đổ ngay vào bồn ngâm đồ vải đã có hóa chất khử khuẩn (Clo hoạt tính ở nồng độ 0,01%-0,05%) trong thời gian tối thiểu là 20 phút trước khi giặt.
Nhân viên thực hiện quy trình giặt tay phải tuân thủ nghiêm ngặt mang trang phục PHCN trong suốt quá trình giặt và sau khi kết thúc tháo bỏ trang phục PHCN và VST.
5.3. Bảo quản và cấp phát đồ vải
- Đồ vải dùng cho người nhiễm hoặc nghi ngờ nhiễm COVID-19 phải được bảo quản trong tủ kín hoặc để vào kệ sạch trong kho, sử dụng theo số lượng và chủng loại nhu cầu.
- Khu vực cách ly, buồng khám người nhiễm hoặc nghi ngờ nhiễm COVID- 19 phải lên danh mục, cơ số đồ vải và báo trước cho nhà giặt.
- Một cơ số đồ vải sạch (ít nhất là cơ số gấp 3) được bảo quản tại khu cách ly để tiện cho việc sử dụng hàng ngày.
6. Kiểm tra và giám sát
- Khoa KSNK, Phòng Điều dưỡng, Trưởng khoa và Điều dưỡng trưởng khoa liên quan có nhiệm vụ huấn luyện, kiểm tra giám sát và đôn đốc việc thực hiện nghiêm túc quy trình thực hiện xử lý đồ vải bẩn (từ phân loại, thu gom, vận chuyển, xử lý).
- Nội dung giám sát:
+ Phương tiện cho xử lý đồ vải bẩn (túi, thùng đựng, xe vận chuyển).
+ Quy trình hướng dẫn và kỹ thuật thực hiện xử lý đồ vải.
+ Rửa tay và vệ sinh các dụng cụ sau khi kết thúc công việc.
+ Hoá chất dùng trong xử lý đồ vải.
+ Phương tiện PHCN cho NVYT.
+ Quy trình sử dụng phương tiện PHCN.
XỬ LÝ DỤNG CỤ ĂN UỐNG
1. Mục đích
- Nhân viên khoa dinh dưỡng tuân thủ đúng quy trình cung cấp và xử lý dụng cụ ăn uống của người nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Bảo đảm an toàn cho NB, NVYT, thân nhân, khách thăm và môi trường.
2. Nguyên tắc thực hiện
- Tất cả đồ dùng sau khi sử dụng cho sinh hoạt, ăn uống và thực phẩm dư thừa của người nhiễm hoặc nghi ngờ nhiễm COVID-19 đều có nguy cơ lây nhiễm cần phải xử lý như chất thải lây nhiễm. Tuyệt đối không được sử dụng vào mục đích khác (tưới cây, nuôi gia súc, gia cầm...).
- Tốt nhất là sử dụng các dụng cụ dùng một lần và sau đó thu gom vận chuyển, tiêu hủy ngay sau khi sử dụng như chất thải y tế lây nhiễm.
- Dụng cụ đựng thức ăn, nước uống dùng riêng cho mỗi NB, thu gom xử lý riêng cho từng NB.
- Trong trường hợp không có dụng cụ dùng một lần, việc tái sử dụng dụng cụ sử dụng phải tuân thủ nghiêm việc khử khuẩn các dụng cụ tái sử dụng giống như quy trình khử khuẩn và tiệt khuẩn các dụng cụ dùng cho chăm sóc và điều trị người nhiễm hoặc nghi ngờ nhiễm COVID-19.
3. Đối tượng và phạm vi áp dụng
Người nhiễm hoặc nghi ngờ nhiễm COVID-19; NVYT; nhân viên khoa dinh dưỡng trực tiếp chăm sóc người nhiễm hoặc nghi ngờ nhiễm COVID-19.
4. Phương tiện
- Phương tiện PHCN phòng lây nhiễm do tiếp xúc.
- Chậu rửa/Lavabo, xà phòng.
- Xô, thùng đựng dung dịch khử khuẩn theo quy định, có nắp đậy chống bay hơi.
- Hóa chất khử khuẩn pha đúng nồng độ 0,05% (500 ppm) Clo hoạt tính.
5. Cách thực hiện
5.1. Sử dụng các dụng cụ dùng một lần
- Người nhiễm hoặc nghi ngờ nhiễm COVID-19 sau khi ăn, uống xong, dụng cụ và thực phẩm còn thừa phải được bỏ vào trong thùng đựng chất thải lây nhiễm trong phòng cách ly.
- Nhân viên vệ sinh thu gom, xử lý chất thải này như chất thải y tế lây nhiễm.
5.2. Sử dụng những dụng cụ tái sử dụng
- NVYT phải hướng dẫn người nhiễm hoặc nghi ngờ nhiễm COVID-19 phải bỏ các dụng cụ sau khi sử dụng xong vào thùng thu gom dụng cụ tái sử dụng, thức ăn thừa cho vào thùng đựng chất thải lây nhiễm.
- NVYT thu gom dụng cụ tái sử dụng đặt vào trong thùng kín có dán nhãn dụng cụ ăn uống của người nhiễm hoặc nghi ngờ nhiễm COVID-19 sau đó chuyển xuống khoa dinh dưỡng (hoặc khoa KSNK) và được xử lý đúng quy trình cho dụng cụ lây nhiễm.
- Khi thực hiện xử lý dụng cụ ăn uống nhân viên cần sử dụng trang phục phòng hộ theo hướng dẫn.
- Các chất lỏng từ thức ăn, nước uống còn thừa, thu gom như chất thải lây nhiễm của khu vực cách ly đúng quy định trước khi vận chuyển đến nơi xử lý.
- Vận chuyển dụng cụ tái sử dụng đến nơi xử lý dụng cụ tập trung, đựng trong túi, thùng có nắp đậy kín an toàn. Không ôm vác trên tay, vai bằng tay trần.
- Ngâm khử khuẩn dụng cụ đựng thức ăn, nước uống sau khi sử dụng trong dung dịch có hoạt chất Clo 0,05% hoạt hóa trong 10 phút - 20 phút. Lưu ý ngâm ngập hoàn toàn dụng cụ trong dung dịch khử khuẩn. Trong trường hợp không có hoá chất khử khuẩn có thể đun sôi 10 phút.
- Khuyến khích sử dụng máy rửa dụng cụ tự động có cửa kín và chạy chu trình hóa chất và nhiệt độ sau đó sấy khô tự động cho các loại dụng cụ (bao gồm nhiều loại dụng cụ khác nhau) dùng cho người nhiễm hoặc nghi ngờ nhiễm COVID-19.
6. Kiểm tra, giám sát
Khoa KSNK, Phòng Điều dưỡng, Trưởng khoa và Điều dưỡng trưởng các khoa liên quan có nhiệm vụ huấn luyện, kiểm tra giám sát và đôn đốc việc thực hiện nghiêm ngặt quy trình:
- Giám sát quy trình sử dụng phương tiện PHCN khi xử lý dụng cụ tái sử dụng.
- Giám sát quy trình thu gom, vận chuyển, xử lý, tái sử dụng.
Xem thêm Hướng dẫn khử khuẩn, tiệt khuẩn trong các cơ sở khám bệnh, chữa bệnh ban hành theo Quyết định số 3671/QĐ-BYT ngày 27/9/2012 của Bộ trưởng Bộ Y tế.
VỆ SINH KHỬ KHUẨN BỀ MẶT MÔI TRƯỜNG
1. Mục đích
- Nhân viên vệ sinh tuân thủ nghiêm ngặt quy trình vệ sinh môi trường khu vực tiếp nhận, điều trị người nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Cắt đứt đường lây truyền qua đường tiếp xúc của COVID-19.
- Đảm bảo an toàn cho NB, NVYT và cộng đồng.
2. Nguyên tắc thực hiện
Bề mặt khu vực sàng lọc, cách ly người nhiễm hoặc nghi ngờ nhiễm COVID- 19 phải được làm sạch, khử khuẩn theo một số nguyên tắc sau:
- Tất cả bề mặt tại khu vực sàng lọc, khu vực cách ly và điều trị nhìn rõ hay không nhìn rõ có dính máu, dịch tiết, chất thải từ người nhiễm hoặc nghi ngờ 1 nhiễm COVID-19 đều phải được làm sạch và lau khử khuẩn tối thiểu ngày 2 lần và khi cần (sau khi khám, làm xét nghiệm, làm thủ thuật, vương vãi máu và dịch, sau chuyển/ra viện, tử vong).
- Tất cả bề mặt (trong khu vực cách ly người nhiễm hoặc nghi ngờ nhiễm COVID-19, bao gồm cả bề mặt các thiết bị chăm sóc, phương tiện vận chuyển phải được làm sạch, lau khử khuẩn bằng các hoá chất khử khuẩn được BYT cấp phép.
- Nhân viên y tế khi thực hiện làm sạch, khử khuẩn các bề mặt liên quan đến người nhiễm hoặc nghi ngờ nhiễm COVID-19 cần tuân thủ nghiêm ngặt nguyên tắc, kỹ thuật vệ sinh bề mặt và các biện pháp phòng ngừa theo đường lây truyền.
- Nhân viên thực hiện làm sạch, khử khuẩn bề mặt môi trường khu vực điều trị, cách ly người nhiễm hoặc nghi ngờ nhiễm COVID-19 phải được tập huấn các quy trình làm sạch, khử khuẩn bề mặt và cách sử dụng đúng đầy đủ phương tiện PHCN khi thực hiện.
3. Đối tượng và phạm vi áp dụng
- Tất cả NVYT làm công tác vệ sinh môi trường ở tất cả các khu vực có liên quan tới chăm sóc, điều trị người nghi ngờ nhiễm hoặc nhiễm COVID-19.
- Tất cả các bề mặt phương tiện, đồ dùng liên quan đến NB, giường, tủ bàn, ghế, nhà vệ sinh... trong khu vực sàng lọc, tiếp nhận, buồng bệnh cách ly, nơi giặt là, thu gom chất thải, nơi xử lý dụng cụ tái sử dụng, phương tiện vận chuyển có liên quan tới chăm sóc, điều trị người nhiễm hoặc nghi ngờ nhiễm COVID-19.
4. Phương tiện
- Phương tiện PHCN (xem phần Sử dụng các phương tiện PHCN).
- Quy trình thực hiện, bảng hướng dẫn pha hoá chất trên xe để phương tiện vệ sinh, khử khuẩn môi trường.
- Xà phòng rửa tay.
- Hóa chất làm sạch và khử khuẩn đã pha theo đúng quy định (có thể dùng dạng xịt cầm tay dùng cho những bề mặt khó lau bằng khăn) có Clo hoạt tính nồng độ 0,05%, khăn lau tẩm dung dịch khử khuẩn hoặc các hóa chất diệt khuẩn thích hợp khác được BYT cấp phép.
- Dung dịch khử khuẩn bề mặt có Clo hoạt tính 0,5% hoặc các hóa chất khử khuẩn khác được Bộ Y tế cấp phép cho vệ sinh bề mặt có đám máu, dịch, chất nôn, chất bài tiết.
- Giẻ lau sạch chuyên cho khu vực sàng lọc và cách ly, cây lau nhà, xô chứa hóa chất và xô gom.
5. Kỹ thuật thực hiện
- Chia khu vực làm hai, có biển báo tránh trơn trượt, ướt trước khi lau vệ sinh sàn nhà, sảnh, cầu thang,
- Lau theo đường zíc zắc, từ trên xuống, từ trong ra ngoài và từ vùng sạch nhất đến vùng kém sạch.
- Khi dùng hóa chất dạng xịt, nên xịt hóa chất vào khăn sau đó lau; nếu lau nền nhà, phun thấp, xịt đến đâu lau đến đó. Không xịt khi có NB.
6. Cách thực hiện
- Bước 1: chuẩn bị đủ phương tiện làm sạch, khử khuẩn (thùng/xô chứa dung dịch khử khuẩn, giẻ lau, cây lau sàn...) sử dụng riêng phương tiện cho các khu vực cách ly (hành chính, buồng bệnh cách ly, khu vệ sinh, khu xử lý dụng cụ, đồ vải...).
- Bước 2: Người thực hiện vệ sinh môi trường mang phương tiện PHCN theo đúng hướng dẫn trước khi vào khu vực cách ly và trong suốt quá trình thực hiện làm sạch, khử khuẩn bề mặt môi trường khu cách ly (xem phần Sử dụng phương tiện PHCN).
- Bước 3: Lau ẩm và thu gom chất thải vào các bao và thùng đựng chất thải lây nhiễm theo đúng quy định trước khi lau khử khuẩn.
- Bước 4: Thực hiện lau khử khuẩn định kỳ bằng dung dịch khuẩn với nồng độ quy định (có nồng độ Clo hoạt tính 0,05%) để khô 10 phút và lau lại nước sạch tránh hoá chất tồn lưu ảnh hưởng tới NB. Tần suất lau ở tất cả các bề mặt trong khu vực cách ly tối thiểu 2 lần/ngày và khi có yêu cầu. Áp dụng đúng quy trình lau 2 xô (một xô nước sạch, một xô dung dịch khử khuẩn) và mỗi lần lau là một giẻ sạch, không giặt lại trong các xô, mỗi giẻ lau không quá 20 m2. Khi lau cần phải chú ý:
+ Với các bề thường xuyên có tiếp xúc (xe tiêm, xe vận chuyển đồ vải dụng cụ, tay nắm cửa...) cần lau khử khuẩn ngay sau mỗi lần sử dụng hoặc có tiếp xúc.
+ Loại bỏ ngay và lau lại bằng dung dịch khử khuẩn có nồng độ Clo hoạt tính 0,5% mỗi khi thấy bề mặt có dính máu, dịch tiết, phân, chất nôn của NB. Thời gian hóa chất tiếp xúc với bề mặt môi trường ít nhất 10 phút.
- Bước 5: Thu gom các dụng cụ sau khi vệ sinh môi trường để làm sạch và khử khuẩn trước khi đưa chúng ra khỏi khu vực buồng bệnh cách ly. Bao gồm chất thải phải được cô lập (xem phần Xử lý chất thải, trang 54), giẻ lau cho vào túi cô lập chuyển xuống nhà giặt (Xem thêm hướng dẫn vận chuyển đồ vải và chất thải, lây nhiễm ra khỏi khu vực cách ly).
- Bước 6: Nhân viên y tế cởi bỏ trang phục PHCN và VST bằng dung dịch xà phòng ngay sau khi kết thúc công việc vệ sinh môi trường.
Lưu ý: Bàn tay NVYT có tiếp xúc trực tiếp với máu, chất tiết, chất thải NB và sau khi tháo phương tiện PHCN phải được rửa tay với xà phòng và nước.
5.1. Vệ sinh khử khuẩn bề mặt hàng ngày
Quy trình thực hiện giống như trên và cần tuân thủ nghiêm ngặt quy định:
- Vệ sinh hai lần mỗi ngày và khi có yêu cầu. Nên có bảng theo dõi các bề mặt đã được khử khuẩn mỗi ngày.
- Với mỗi lần vệ sinh, cần lau khử khuẩn các bề mặt bằng hóa chất khử khuẩn trước khi lau lại bằng dung dịch làm sạch, cần thực hiện vệ sinh khử khuẩn từ khu vực ít ô nhiễm (khu vực hành chính) tới khu vực ô nhiễm nhiều (buồng cách ly), các bề mặt phương tiện thiết bị trước khi khử khuẩn và làm sạch sàn nhà.
- Sử dụng hóa chất khử khuẩn diệt được COVID-19 cho tất cả các bề mặt trong phòng và bảo đảm đúng thời gian tiếp xúc với hóa chất khử khuẩn. Ví dụ ít nhất 10 phút với các hợp chất có Clo hoạt tính 0,05% (500 ppm).
Lưu ý: không mang các dụng cụ vệ sinh tại khu vực cách ly ra nơi khác, tải lau được thu gom xử lý riêng tránh lây nhiễm COVID-19 ra khu vực khác trong bệnh viện.
5.2. Vệ sinh sau khi người bệnh ra viện/chuyển viện/tử vong
- Chuyển NB cách ly khác trong buồng bệnh (nếu có) sang buồng cách ly khác trước khi thực hiện vệ sinh khử khuẩn lần cuối.
- Thu gom các dụng cụ bẩn, đồ vải tái sử dụng vào các thùng/túi theo quy định về trung tâm tiệt khuẩn, giặt là. Thu gom và loại bỏ chất thải và các vật dụng cá nhân khác của NB theo quy định thu gom và quản lý chất thải lây nhiễm.
- Lau khử khuẩn các bề mặt bằng hóa chất khử khuẩn trước khi lau lại bằng dung dịch làm sạch, cần thực hiện vệ sinh khử khuẩn từ khu vực ít ô nhiễm (khu vực hành chính) tới khu vực ô nhiễm nhiều (buồng cách ly), các bề mặt phương tiện thiết bị trước khi khử khuẩn và làm sạch sàn nhà.
- Sử dụng hóa chất khử khuẩn diệt được COVID-19 cho tất cả các bề mặt trong phòng và bảo đảm đúng thời gian tiếp xúc với hóa chất khử khuẩn, ví dụ ít nhất 10 phút với các dung dịch có Clo hoạt tính 0,05%-0,5%.
Chi tiết về nồng độ hóa chất sử dụng trong vệ sinh, khử khuẩn bề mặt tại Phụ lục 4
5.3. Vệ sinh khử khuẩn bề mặt đề tràn máu hoặc dịch cơ thể
- Cần thực hiện ngay khi xuất hiện hoặc ngay khi được phát hiện đám máu hoặc dịch cơ thể.
- Mang đầy đủ phương tiện PHCN.
- Loại bỏ đám máu hoặc dịch cơ thể theo trình tự: (1) Dùng khăn hoặc gạc tẩm dung dịch chứa 0,5% (5.000 ppm) Clo hoạt tính loại bỏ đám máu (nếu lượng, máu tràn nhiều phải thực hiện nhiều lần đến khi loại bỏ hết máu trên bề mặt; (2) Loại bỏ khăn (gạc) đã thấm máu vào thùng thu gom chất thải lây nhiễm; (3) Dùng khăn hoặc gạc tẩm dung dịch chứa 0,5% Clo hoạt tính lau khử khuẩn bề mặt khu vực tràn máu; (4) Dùng khăn hoặc gạc tẩm dung dịch làm sạch lau lại bề mặt vừa khử khuẩn.
- Cởi bỏ phương tiện PHCN và VST sau khi ra khỏi phòng cách ly.
5.4. Vệ sinh môi trường nhà đại thể và khu vực khâm liệm người bệnh COVID-19
- Mang đầy đủ phương tiện phòng hộ theo quy định đối với COVID-19.
- Sau khi khâm liệm, phẫu thuật tử thi hoàn tất, tất cả dụng cụ, bề mặt bàn phẫu thuật, buồng phẫu thuật, phương tiện liên quan đến tử thi phải được khử khuẩn ngay bằng dung dịch Clo hoạt tính 0,5% và để khô từ 30 phút đến 1 giờ.
- Làm sạch và khử khuẩn phương tiện vệ sinh theo quy trình.
- Cởi bỏ phương tiện PHCN và VST sau khi kết thúc công việc.
5.5. Vệ sinh làm sạch dụng cụ vệ sinh
- Dụng cụ vệ sinh bệnh viện phải được làm sạch sau mỗi ca làm việc, cuối mỗi ngày.
- Các dụng cụ vệ sinh được xử lý bao gồm, cán cây lau nhà, xô/chậu đựng hóa chất, nước xả/ngâm khử khuẩn tấm lau được làm sạch, đánh chải với nước sạch và xà phòng để đúng nơi quy định, khô ráo.
- Khử nhiễm các chậu/xô đựng dung dịch tẩy rửa và khử khuẩn ở nồng độ Clo hoạt tính 0,05%, rửa lại với nước sạch úp trên giá bảo quản làm khô.
- Thu dọn dụng cụ vệ sinh để đúng nơi quy định. Không sử dụng dụng cụ vệ sinh chưa được xử lý để làm vệ sinh hàng ngày.
6. Kiểm tra, giám sát
- Khoa KSNK, Phòng Điều dưỡng, Trưởng khoa và Điều dưỡng trưởng các khoa liên quan có nhiệm vụ huấn luyện, kiểm tra giám sát và đôn đốc việc thực hiện nghiêm ngặt quy trình vệ sinh khử khuẩn môi trường hàng ngày hoặc đột xuất.
- Giám sát hàng ngày sự tuân thủ của NVYT về thực hiện quy trình khử khuẩn làm sạch bề mặt, khử khuẩn sự cố tràn máu, dịch tiết sinh học, sử dụng phương tiện PHCN, vệ sinh khi làm việc trong khu vực cách ly điều trị người nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Kết quả giám sát cần phản hồi ngay cho người được giám sát và báo cáo cho lãnh đạo khoa, lãnh đạo bệnh viện.
Xem thêm Hướng dẫn vệ sinh môi trường bề mặt trong các cơ sở khám bệnh, chữa bệnh ban hành theo Quyết định số 3916/QĐ-BYT ngày 28/8/2017 của Bộ trưởng Bộ Y tế.
VỆ SINH PHƯƠNG TIỆN VẬN CHUYỂN NGƯỜI NHIỄM HOẶC NGHI NGỜ NHIỄM COVID-19
Các bệnh viện phải áp dụng một cách nghiêm ngặt các quy trình kỹ thuật và các nguyên tắc kiểm soát môi trường, kiểm soát thực hành an toàn trong sử dụng phương tiện PHCN khi vận chuyển người bệnh trong và ngoài bệnh viện.
1. Mục đích
- Nhân viên y tế thực hành đúng và nghiêm ngặt quy định vệ sinh, khử khuẩn bề mặt phương tiện vận chuyển người nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Phòng ngừa lây nhiễm COVID-19 do tiếp xúc với bề mặt các phương tiện vận chuyển người nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Đảm bảo an toàn cho NVYT vận chuyển và cộng đồng.
2. Nguyên tắc thực hiện
- Các bề mặt phương tiện vận chuyển cần vệ sinh, khử khuẩn gồm: khoang bên trong xe vận chuyển NB (cáng, bảng điều khiển thiết bị y tế, sàn liền kề, tường, trần và bề mặt làm việc, tay nắm cửa, radio, bàn phím và điện thoại) và bề mặt bên ngoài xe vận chuyển (tay nắm cửa, cửa, toàn bộ bề mặt bên ngoài xe).
- Người thực hiện xử lý phương tiện vận chuyển (là người trực tiếp tham gia vận chuyển hoặc người được phân công làm nhiệm vụ vệ sinh vận chuyển xe sau cùng) phải được huấn luyện và thực hiện đúng nguyên tắc và kỹ thuật vệ sinh bề mặt máy móc, phương tiện và xe vận chuyển, các biện pháp phòng ngừa chuẩn và phòng ngừa lây truyền theo đường tiếp xúc.
- Bệnh viện có quy định nơi xử lý phương tiện vận chuyển và trang bị đầy đủ phương tiện đảm bảo xử lý an toàn phương tiện.
- Nơi thực hiện xử lý khử khuẩn phương tiện vận chuyển NB phải có đầy đủ phương tiện PHCN, hoá chất, dụng cụ làm vệ sinh, khử khuẩn tiệt khuẩn, thu gom chất thải y tế.
- Tất cả phương tiện vận chuyển NB, dụng cụ can thiệp, chăm sóc NB sau khi kết thúc sử dụng phải được xử lý ngay theo đúng quy trình trước khi sử dụng cho những NB tiếp theo.
3. Đối tượng và phạm vi áp dụng
- Tất cả các phương tiện vận chuyển NB đến bệnh viện và trong khuôn viên bệnh viện.
- Tất cả NVYT tham gia vào vận chuyển NB tại tất cả các khoa phòng có liên quan đến vận chuyển người nhiễm hoặc nghi ngờ nhiễm COVID-19.
4. Phương tiện
- Phương tiện PHCN: có đủ bộ phương tiện PHCN, khẩu trang N95, khẩu trang y tế, kính bảo hộ hoặc tâm che mặt, ủng cao su, găng tay sạch, găng tay vô khuẩn khi làm thủ thuật xâm lấn rời để có thể thay thế và sử dụng khi cần.
- Hóa chất làm sạch và khử khuẩn:
+ Xà phòng có chất khử khuẩn
+ Dung dịch VST có chứa cồn.
+ Dung dịch khử khuẩn bề mặt có hoạt chất Clo hoạt tính 0,05% và 0,5%, con ethanol 70 độ hoặc các chất khử khuẩn trong danh mục cấp phép của BYT.
- Phương tiện để xử lý: bình phun, giẻ lau, túi/bao đựng chất thải
- Khu vực xử lý các xe vận chuyển riêng trong khuôn viên bệnh viện.
5. Cách thực hiện
NVYT mang trang phục PHCN đúng hướng dẫn và thực hiện theo các bước sau:
- Bước 1: Pha hóa chất đúng quy định và để vào trong các bình đựng hóa chất sẵn tại khu vực xử lý.
- Bước 2: Mang phương tiện PHCN.
- Bước 3: Thu gom các dụng cụ và chất thải cho vào các bao/túi màu vàng và gói kín, ghi rõ chất thải phát sinh từ chuyển đến nơi xử lý chất thải tập trung.
- Bước 4: Lau hóa chất khử khuẩn lên tất cả bề mặt phương tiện vận chuyển, để ít nhất 10 phút sau đó lau lại với chất làm sạch (chất tẩy rửa hoặc nước sạch với xà phòng), lau khô hoặc xì khô. Khi có nhiều máu, dịch hoặc có sự có đổ tràn máu hoặc tràn dịch cơ thể (VD: chất nôn, máu, dịch tiết sinh học...), trước tiên phải dùng khăn giấy thấm dùng một lần có tẩm Clo hoạt tính 0,5% khu trú lại và loại bỏ, dùng khăn tẩm dung dịch Clo hoạt tính 0,5% phủ lên khu vực đổ tràn để trong ít nhất 10 phút, sau đó lau sạch lại với dung dịch bằng dung dịch khử khuẩn Clo hoạt tính 0,05%.
- Bước 5: Sau khi kết thúc công việc, phương tiện bảo hộ cá nhân được cho vào túi hoặc thùng có nắp kín, chuyển tới nơi khử khuẩn hoặc tiêu hủy, rửa tay bằng xà phòng có chất khử khuẩn và vệ sinh cá nhân.
Chú ý: Đối với các phương tiện ô tô đi đến vùng dịch cần được phun hoá chất khử khuẩn, thân, lốp, gầm xe khi rời khỏi vùng dịch bằng dung dịch khử khuẩn có nồng độ 0,05% Clo hoạt tính.
6. Kiểm tra, giám sát và trách nhiệm
- Khoa KSNK, Phòng Điều dưỡng, Trưởng khoa và Điều dưỡng trưởng các khoa liên quan có nhiệm vụ huấn luyện, kiểm tra giám sát và đôn đốc việc thực hiện nghiêm ngặt quy trình vệ sinh xe vận chuyển người nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Phòng Kế hoạch tổng hợp cùng Khoa HSCC kiểm tra phương tiện cấp cứu, xe cấp cứu và quy chế cấp cứu trong phòng chống dịch - thiên tai.
- Phòng Vật tư - Trang thiết bị, khoa Dược (hoặc đơn vị được giao nhiệm vụ cung cấp) có trách nhiệm cung cấp đầy đủ phương tiện PHCN và các hóa chất khử khuẩn, tiệt khuẩn trong danh mục BYT cho phép.
- Khoa KSNK thực hiện giám sát tuân thủ quy trình vệ sinh khử khuẩn phương tiện, xử lý chất thải y tế và vệ sinh môi trường nơi thực hiện vệ sinh khử khuẩn phương tiện.
XỬ LÝ CHẤT THẢI
1. Mục đích
- Nhân viên, người nhiễm hoặc nghi ngờ nhiễm thực hiện đúng quy trình phân loại, cô lập, thu gom, vận chuyển và xử lý chất thải phát sinh từ khu vực cách ly.
- Ngăn ngừa phát tán COVID-19 từ chất thải ra môi trường và cộng đồng.
- Bảo đảm an toàn cho NB, NVYT và cộng đồng.
2. Nguyên tắc
- Tất cả chất thải phải được thu gom xử lý ngay tại nơi phát sinh từ khu vực sàng lọc, khu vực cách ly của người nhiễm hoặc nghi ngờ nhiễm COVID-19 đều được coi là chất thải lây nhiễm, cần được thu gom trong túi ni-lon và thùng kín màu vàng có biểu tượng nguy hại sinh học.
- Bảo đảm không phát tán mầm bệnh trong quá trình thu gom, vận chuyển và xử lý chất thải y tế từ khu vực sàng lọc, khu vực cách ly của người nhiễm hoặc nghi ngờ nhiễm COVID-19; bảo đảm an toàn cho NVYT và người tham gia quản lý chất thải y tế.
- Chất thải y tế khi đưa ra ngoài phải cho vào một túi chất thải màu vàng trước khi chuyển xuống nhà chứa chất thải tập trung của bệnh viện, ghi cảnh báo “Chất thải có nguy cơ chứa COVID-19”.
- Nhân viên y tế và người tham gia quản lý chất thải y tế, vệ sinh môi trường phải được trang bị đầy đủ phương tiện bảo vệ cá nhân phù hợp khi đang làm việc.
3. Phạm vi áp dụng
3.1. Đối tượng
- Nhân viên làm nhiệm vụ thu gom, vận chuyển và xử lý chất thải người nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Tất cả NVYT tham gia vào quá trình chăm sóc điều trị người nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Người nhiễm hoặc nghi ngờ nhiễm COVID-19, người nhà NB, khách thăm.
3.2. Khu vực
- Tại tất cả những nơi có người nhiễm hoặc nghi ngờ nhiễm COVID-19 làm phát sinh chất thải: tiếp nhận, khám sàng lọc, khu vực cách ly, xét nghiệm... người nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Khu vực xử lý chất thải.
4. Phương tiện
- Thùng và túi ni-lon dùng cho thu gom chất thải y tế lây nhiễm theo đúng quy định (màu vàng) có biểu tượng chất thải lây nhiễm theo quy định được đặt trong khu vực sàng lọc, phòng cách ly, phòng bệnh và buồng đệm.
- Trên xe tiêm hoặc trong phòng cách ly được trang bị hộp thu gom chất thải sắc nhọn (màu vàng, kháng thủng, sử dụng một lần).
- Trên xe chuyển người nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Phương tiện bảo hộ (mũ, khẩu trang, kính bảo hộ, quần áo, ủng cao su/bao giây) cho người thu gom, xử lý, quản lý chất thải y tế.
5. Biện pháp thực hiện
- Chất thải là bệnh phẩm của người nghi ngờ nhiễm hoặc nhiễm COVID-19 phải được xử lý an toàn theo hướng dẫn xử lý chất thải có nguy cơ lây nhiễm cao trước khi đưa vào hệ thống xử lý tập trung.
- Tất cả chất thải rắn phát sinh trong khu vực khám sàng lọc, khu cách ly và khu vực có liên quan đến người nhiễm hoặc nghi ngờ nhiễm COVID-19 phải được thu gom ngay vào thùng, hộp hoặc túi thu gom chất thải lây nhiễm.
- Thùng đựng chất thải lây nhiễm tại nơi lưu giữ tạm thời phải được đậy nắp kín, bảo đảm không bị rơi, rò rỉ chất thải trong quá trình thu gom về khu lưu giữ tập trung trong khuôn viên của cơ sở y tế ít nhất 2 lần/ngày.
- Nhân viên thu gom, vận chuyển chất thải mang phương tiện phòng hộ theo đúng quy định.
- Chất thải phải được vận chuyển đến nơi tập trung chất thải của bệnh viện khi thùng chứa đầy 3/4 trở lên hoặc ít nhất 2 lần/ngày và khi có yêu cầu.
|
- Trước khi vận chuyển tới nơi tập trung chất thải của bệnh viện, chất thải phải được gói kín trong túi ni-lon màu vàng ngay trong buồng cách ly và dán nhãn “Chất thải có nguy cơ chứa COVID-19” sau đó đặt vào một túi thu gom khác bên ngoài buồng cách ly. - Khi đã chuyển chất thải tới nơi tập trung chất thải của bệnh viện, chất thải được xử lý tiêu huỷ tập trung như những chất thải lây nhiễm cao khác. Tuyệt đối không mở túi chất thải này khi lưu giữ, vận chuyển và xử lý. |
|

- Chất thải lỏng như phân, nước tiểu phát sinh từ buồng cách ly hoặc khu vực cách ly cần được thu gom theo hệ thống thu gom và xử lý nước thải y tế chung của bệnh viện. Trường hợp cơ sở chưa có hệ thống xử lý nước thải đạt tiêu chuẩn môi trường, chất thải lỏng từ khu vực cách ly phải được thu gom và xử lý khử khuẩn băng dung dịch hoá chất chứa 1,0% Clo hoạt tính trước khi thải ra môi trường.
- Chất tiết đường hô hấp (đờm, rãi, dung dịch họng, dịch phế quản của NB phải được xử lý triệt để bằng dung dịch 1,0 % Clo hoạt tính với tỷ lệ 1:1 trong thời gian ít nhất 10 phút sau đó thu gom theo quy định của đơn vị điều trị.
- Tại các đơn vị có lò hấp nhiệt độ cao chất thải rắn và bệnh phẩm phát sinh từ phòng xét nghiệm cần được hấp ở nhiệt độ 121°C trong 20 phút trước khi tập trung chất thải và xử lý theo quy định.
- Vận chuyển, xử lý tập trung: Thùng đựng chất thải lây nhiễm phải đáp ứng đúng quy định tại Thông tư liên tịch số 58/2015/TTLT-BYT-BTNMT ngày 31/12/2015 của BYT và BTN&MT quy định về quản lý chất thải y tế và có dán nhãn “Chất thải có nguy cơ chứa COVID-19”, có thành cứng, có nắp đậy kín, có lắp bánh xe đẩy. Chất thải lây nhiễm phải được vận chuyển và xử lý ngay trong ngày. Thời điểm và lối đi vận chuyển chất thải nên tránh đông người.
- Đồ vải, quần áo thải bỏ của người nhiễm hoặc nghi ngờ nhiễm COVID-19, trang phục PHCN của NVYT và người tham gia quản lý chất thải y tế, vệ sinh môi trường tại khu vực sàng lọc, theo dõi, cách ly, chăm sóc, điều trị người nhiễm hoặc nghi ngờ nhiễm COVID-19 phải được thu gom và xử lý như chất thải lây nhiễm nêu trên.
6. Kiểm tra và giám sát
- Khoa KSNK, Phòng Điều dưỡng, Trưởng khoa và Điều dưỡng trưởng các khoa liên quan có nhiệm vụ huấn luyện, kiểm tra giám sát và đôn đốc việc thực hiện nghiêm ngặt quy trình xử lý chất thải người nhiễm hoặc nghi ngờ nhiễm COVID-19. Nội dung giám sát:
+ Phương tiện thu gom vận chuyển.
+ Thực hành phân loại, thu gom, vận chuyển và tiêu huỷ.
+ Khối lượng chất thải phát sinh.
- Báo cáo ngay cho các trưởng khoa, điều dưỡng trưởng, Ban phòng chống dịch COVID-19 và lãnh đạo bệnh viện khi có sự cố hoặc bất kỳ vấn đề gì có liên quan đến phát tán nguồn nhiễm từ chất thải.
LẤY, BẢO QUẢN, ĐÓNG GÓI VÀ VẬN CHUYỂN BỆNH PHẨM
Tất cả bệnh phẩm sinh học từ người nhiễm hoặc nghi ngờ nhiễm COVID-19 đều là nguồn lây nhiễm tiềm tàng và nguy hiểm cho người lấy mẫu, thu thập, vận chuyển và xử lý. Việc tuân thủ nghiêm ngặt quy định về an toàn sinh học cấp độ 2 là bắt buộc khi có tiếp xúc, xử lý nguồn bệnh phẩm này.
1. Mục đích
- Phòng ngừa lây nhiễm COVID-19 qua tiếp xúc từ các loại bệnh phẩm và những người tiếp xúc với NB trong quá trình lấy, bảo quản, đóng gói và vận chuyển, xử lý và làm các xét nghiệm (XN) liên quan đến bệnh phẩm người nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Tất cả nhân viên lấy mẫu đều thực hiện đúng và nghiêm ngặt quy trình và quy định khi lấy mẫu, bảo quản và vận chuyển mẫu của người nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Tránh phát tán nguồn bệnh, bảo đảm an toàn cho NVYT và môi trường.
2. Nguyên tắc thực hiện
Phòng ngừa lây nhiễm do tiếp xúc là ưu tiên hàng đầu trong quá trình lấy, bảo quản, đóng gói và vận chuyển, xử lý và làm các XN liên quan đến bệnh phẩm của người nhiễm hoặc nghi ngờ nhiễm COVID-19.
2.1. Yêu cầu về người lấy, bảo quản, đóng gói và vận chuyển bệnh phẩm của người nghi ngờ nhiễm hoặc nhiễm COVID-19
Người lấy, bảo quản, đóng gói, vận chuyển, xử lý và làm các XN liên quan đến bệnh phẩm của người nhiễm hoặc nghi ngờ nhiễm COVID-19 phải là NVYT đã được đào tạo, có kỹ năng thực hành thành thạo các hướng dẫn phòng ngừa lây nhiễm.
- Tuân thủ nghiêm ngặt các quy định về an toàn sinh học trong thu thập, bảo quản, đóng gói và vận chuyển, xử lý và làm các XN liên quan đến bệnh phẩm lây qua đường máu, lây truyền các tác nhân qua đường không khí và đường tiếp xúc.
- Sử dụng phương tiện PHCN thành thạo, đúng quy định.
- Hiểu được nguy cơ lây nhiễm, có khả năng phát hiện và đánh giá nguy cơ cho cá nhân, có kiến thức kiểm soát sức khoẻ sau khi làm nhiệm vụ và tự xử lý được theo đúng quy trình khi bị phơi nhiễm.
- Tốt nhất là các NVYT đang theo dõi và chăm sóc NB nghi ngờ thực hiện lấy bệnh phẩm, hạn chế tối đa số người tiếp xúc với NB.
2.2. Yêu cầu về dụng cụ
Tất cả các dụng cụ sử dụng để lấy, bảo quản, đóng gói và vận chuyển bệnh phẩm và tất cả dụng cụ XN, bệnh phẩm thừa của người nghi ngờ nhiễm hoặc nhiễm COVID-19 đều là chất thải có nguy cơ lây nhiễm cao, phải được xử lý khử khuẩn tại khoa XN trước khi trở thành chất thải y tế lây nhiễm.
- Ưu tiên sử dụng các dụng cụ sử dụng một lần, tiêu huỷ ngay sau khi sử dụng như chất thải lây nhiễm.
- Dụng cụ nếu tái sử dụng lại phải được khử khuẩn, tiệt khuẩn đúng quy định, phải có bồn xử lý riêng tránh lây nhiễm sang dụng cụ của NB khác.
- Dụng cụ dùng riêng cho mỗi NB phải thu gom xử lý riêng.
2.3. Yêu cầu về khu vực lấy mẫu và xét nghiệm
- Khu vực lấy mẫu và làm XN phải là khu vực cách ly.
3. Đối tượng và phương pháp áp dụng
- Nhân viên y tế tuân thủ nghiêm ngặt các quy định về an toàn sinh học, phải sử dụng phương tiện PHCN theo quy định thành thạo.
- Người nhiễm hoặc nghi ngờ nhiễm COVID-19 phải ở khu vực cách ly.
- Dụng cụ lấy bệnh phẩm, dụng cụ XN và bệnh phẩm thừa của người nhiễm hoặc nghi ngờ nhiễm COVID-19 sau khi làm xong XN phải được xử lý như chất thải y tế có nguy cơ lây nhiễm cao.
4. Phương tiện
4.1. Phương tiện phòng hộ cá nhân
- Bộ quần áo chống dịch sử dụng một lần.
- Tấm choàng không thấm nước.
- Mũ trùm hoặc tấm choàng che kín đầu, cổ bằng chất liệu không thấm nước.
- Khẩu trang có hiệu lực lọc cao (ví dụ N95), hoặc khẩu trang có bộ phận lọc và hỗ trợ thở (tăng cường oxy thở).
- Kính bảo hộ hoặc tấm che mặt.
- Găng tay đeo hai lớp, lớp một (lớp bên trong) là găng tay y tế luôn giữ sạch, tránh không để tiếp xúc với dụng cụ bẩn.
- Ủng cao su/giầy chống thấm cổ cao.
- Dung dịch VST chứa cồn/xà phòng VST.
4.2. Dụng cụ lấy bệnh phẩm
- Tăm bông cán mềm, cán cứng vô trùng.
- Đè lưỡi.
- Bệnh phẩm thu thập được chứa trong ống môi trường vận chuyển vi rút (VTM, UTM) có 3ml môi trường.
4.2.1. Mẫu bệnh phẩm hô hấp:
- Dịch tỵ hầu: tăm bông cán mềm vô trùng (theo quy định của Phòng XN).
- Dịch ngoáy họng: tăm bông cán cứng vô trùng lấy bệnh phẩm (theo quy định phòng XN).
- Dịch súc họng: nước muối sinh lí, cốc nhựa vô trùng (bệnh phẩm được thu thập vào cốc hoặc đĩa petri và pha loãng trong môi trường vận chuyển mẫu theo quy định phòng XN).
- Dịch nội khí quản/dịch phế quản/phế nang/màng phổi: dụng cụ chuyên dụng.
4.2.2. Mẫu bệnh phẩm máu:
- Bơm tiêm 10ml vô trùng.
- Tuýp lấy máu có hoặc không có chất chống đông (yêu cầu của phòng XN)
- Dây garo, bông, cồn...
4.2.3. Đóng gói bệnh phẩm:
- Hộp nhựa có nắp vặn kín, giá nhựa hoặc túi ni-lon để đóng gói bệnh phẩm.
- Bình lạnh bảo quản mẫu, thùng vận chuyển mẫu.
- Băng gạc có tẩm chất sát trùng (xử lý tràn, bắn mẫu bệnh phẩm)
4.3. Thông tin trên ống chứa bệnh phẩm
- Tên người bệnh (hoặc mã số bệnh phẩm).
- Tuổi.
- Ngày thu thập mẫu, thời gian thu thập mẫu.
- Loại bệnh phẩm.
4.4. Phiếu yêu cầu xét nghiệm và phiếu điều tra dịch tễ
Điền đầy đủ thông tin (theo biểu mẫu quy định tại Quyết định 343/QĐ-BYT ngày 07/02/2020 ban hành Hướng dẫn tạm thời giám sát và phòng, chống bệnh viêm đường hô hấp cấp do chủng mới của vi rút Corona).
5. Các bước thực hiện
5.1. Mang phương tiện phòng hộ cá nhân
Mang phương tiện PHCN đúng quy định (xem phần Sử dụng phương tiện PHCN). Chú ý mang khuẩn trang N95 và mang 2 lớp găng tay khi lấy bệnh phẩm.
5.2. Quy định về lấy bệnh phẩm
5.2.1. Mẫu bệnh phẩm
Bệnh phẩm thu thập bắt buộc phải lấy tối thiểu 01 mẫu bệnh phẩm đường hô hấp, có thể lấy thêm 01 mẫu máu; các loại mẫu dưới đây:
- Bệnh phẩm đường hô hấp trên:
+ Dịch tỵ hầu và dịch ngoáy họng.
+ Dịch súc họng.
- Bệnh phẩm đường hô hấp dưới:
+ Đờm
+ Dịch phế nang, dịch nội khí quản, dịch màng phổi...
+ Tổ chức phổi, phế quản, phế nang (khi có chỉ định).
- Mẫu máu: 3-5 ml máu tĩnh mạch có hoặc không có chất chống đông EDTA. Huyết thanh hoặc huyết tương lưu mẫu theo yêu cầu của phòng XN (thực hiện xét nghiệm theo yêu cầu)
5.2.2. Thời điểm thu thập bệnh phẩm
Thời điểm thu thập bệnh phẩm đường hô hấp nên được thực hiện sớm nhất sau khi khởi phát.
Bảng 2. Thời điểm thu thập bệnh phẩm xét nghiệm xác định COVID-19
|
Loại bệnh phẩm |
Thời điểm thu thập thích hợp |
|
Bệnh phẩm đường hô hấp trên (dịch mũi họng, dịch súc họng) |
Tại ngày 0 đến ngày 7 sau khi khởi bệnh |
|
Bệnh phẩm đường hô hấp dưới (dịch phế nang, dịch nội khí quản, dịch màng phổi...) |
Tại ngày 0 đến ngày 14 sau khi khởi bệnh |
|
Mẫu máu giai đoạn cấp |
Cùng thời điểm bệnh phẩm hô hấp trên (tại ngày 0 đến ngày 7 sau khi khởi bệnh) |
|
Mẫu máu giai đoạn hồi phục |
Tại ngày 14, 28 hoặc 3 tháng sau khi khởi bệnh |
|
Tổ chức phế nang |
Trong trường hợp có chỉ định |
5.2.3. Kỹ thuật lây bệnh phẩm
5.2.3.1 Dịch ty hầu và dịch ngoáy họng (sử dụng 02 tăm bông cho 02 loại bệnh phẩm), lấy đồng thời dịch ngoáy họng và dịch tỵ hầu của bệnh nhân
a. Dịch ngoáy họng
- Yêu cầu bệnh nhân há miệng to.
- Dùng dụng cụ đè nhẹ nhàng lưỡi NB.
- Đưa tăm bông vào vùng hầu họng, miết và xoay tròn nhẹ 3-4 lần tại khu vực 2 bên vùng A-mi-đan và thành sau họng để lấy được dịch, tế bào vùng họng.
- Sau khi lấy bệnh phẩm, que tăm bông được chuyển vào ống chứa 3ml môi trường vận chuyển (VTM hoặc UTM) để bảo quản. Lưu ý, đầu tăm bông phải nằm ngập hoàn toàn trong môi trường vận chuyển, và nếu que tăm bông dài hơn ống đựng môi trường vận chuyển cần bẻ/cắt cán tăm bông cho phù hợp với độ dài của ống nghiệm chứa môi trường vận chuyển.
b. Dịch tỵ hầu
- Yêu cầu NB ngồi yên, mặt hơi ngửa, trẻ nhỏ thì phải có người lớn giữ.
- Người lấy bệnh phẩm nghiêng đầu bệnh nhân ra sau khoảng 70°, tay đỡ phía sau cổ NB.
- Tay kia đưa nhẹ nhàng tăm bông vào mũi, vừa đẩy vừa xoay giúp tăm bông đi dễ dàng vào sâu 1 khoảng bằng 1/2 độ dài từ cánh mũi đến dái tai cùng phía.
Lưu ý: nếu chưa đạt được độ sâu như vậy mà cảm thấy có lực cản rõ thì rút tăm bông ra và thử lấy mũi bên kia. Khi cảm thấy tăm bông chạm vào thành sau họng mũi thì dừng lại, xoay tròn rồi từ từ rút tăm bông ra
- Giữ tăm bông tại chỗ lấy mẫu trong vòng 5 giây để đảm bảo dịch thấm tối đa.
- Từ từ xoay và rút tăm bông ra.
- Đặt đầu tăm bông vào ống đựng bệnh phẩm có chứa môi trường vận chuyển và bẻ cán tăm bông tại điểm đánh dấu để có độ dài phù hợp với độ dài của ống nghiệm chứa môi trường vận chuyển. Que tăm bông sau khi lấy dịch ngoáy mũi sẽ được để chung vào ống môi trường chứa que tăm bông lấy dịch ngoáy họng.
- Đóng nắp, xiết chặt, bọc ngoài bằng giấy parafin (nếu có).
Bảo quản mẫu trong điều kiện nhiệt độ 2-8°C trước khi chuyển về phòng xét nghiệm. Nếu bệnh phẩm không được vận chuyển đến phòng XN trong vòng 48 giờ kể từ khi lấy mẫu, các mẫu bệnh phẩm phải được bảo quản trong âm 70°C (-70°C).
Lưu ý: Đối với trẻ nhỏ đặt ngồi trên đùi của cha/mẹ, lưng của trẻ đối diện với phía ngực cha mẹ. Cha/mẹ cần ôm trẻ giữ chặt cơ thể và tay trẻ. Yêu cầu cha/mẹ ngả đầu trẻ ra phía sau.
5.2.3.2 Dịch súc họng
Người bệnh được súc họng với 10 ml dung dịch rửa (nước muối sinh lý). Dịch súc họng được thu thập vào cốc hoặc đĩa petri và pha loãng theo tỷ lệ 1:2 trong môi trường bảo quản vi rút.
5.2.3.3 Dịch nội khí quản
Người bệnh khi đang thở máy, đã được đặt nội khí quản. Dùng 1 ống hút dịch, đặt theo đường nội khí quản và dùng bơm tiêm hút dịch nội khí quản theo đường ống đã đặt, cho dịch nội khí quản vào ống chứa môi trường bảo quản vi rút.
5.2.3.4 Lấy mẫu máu:
Sử dụng bơm kim tiêm vô trùng lấy 3ml-5ml máu tĩnh mạch, chuyển vào tuýp chứa (có hoặc không có chất chống đông EDTA), bảo quản ở nhiệt độ 4°C trong vòng 24 giờ.
Lưu ý:
- Ghi rõ tên, tuổi, địa chỉ, của NB loại bệnh phẩm, ngày lấy mẫu trên tuýp đựng bệnh phẩm
- Các loại bệnh phẩm thu thập tại đường hô hấp dưới (dịch nội khí quản, phế nang, màng phổi) phải được phối hợp với các bác sỹ lâm sàng trong quá trình thu thập mẫu bệnh phẩm.
5.2.4. Khử khuẩn dụng cụ và khu vực lấy mẫu
- Dụng cụ lấy mẫu, phương tiện PHCN xử lý như chất thải lây nhiễm.
- Khu vực lấy mẫu được khử khuẩn bề mặt như buồng cách ly.
5.3. Quy định về bảo quản bệnh phẩm
Bệnh phẩm sau khi thu thập được chuyển đến phòng xét nghiệm trong thời gian ngắn nhất:
- Bệnh phẩm được bảo quản tại 2°C-8°C, và chuyển tới phòng XN trong thời gian sớm nhất, đảm bảo không quá 48 giờ sau khi thu thập.
- Bệnh phẩm được bảo quản ngay tại -70°C trong trường hợp thời gian dự kiến chuyển đến phòng XN chậm hơn 48 giờ sau khi thu thập.
- Không bảo quản bệnh phẩm tại ngăn đá của tủ lạnh hoặc -20°C.
5.4. Quy định về đóng gói bệnh phẩm
Bệnh phẩm khi vận chuyển phải được đóng gói theo nguyên tắc 3 lớp để đảm bảo an toàn sinh học.
- Theo Thông tư 40/2018/TT-BYT về quản lý mẫu bệnh phẩm.
5.4.1. Đóng gói bệnh phẩm để vận chuyển làm xét nghiệm thường quy
- Lớp trong cùng: lọ chứa mẫu bệnh phẩm theo đúng quy định của phòng XN cung cấp. Không để bệnh phẩm bị tràn vãi ra ngoài.

Hình 13. Đóng gói bệnh phẩm (ba lớp) để vận chuyển trong bệnh viện làm xét nghiệm thường quy
- Lớp giữa: giá nhựa, giá xốp, hộp nhựa để giữ cho bệnh phẩm thẳng đứng.
- Lớp ngoài cùng: hộp nhựa cứng, có nắp đậy và quai xách, trên hộp phải có dán nhãn nguy hại sinh học.
5.4.2. Đóng gói bệnh phẩm để vận chuyển đi xa làm xét nghiệm khẳng định COVID-19
Bệnh phẩm khi vận chuyển phải được đóng gói kỹ trong 3 lớp bảo vệ, theo hướng dẫn của Tổ chức Y tế thế giới.
- Tuýp chứa môi trường vận chuyển: chứa mẫu trực tiếp. Tuýp nhựa có nắp kín, đóng nắp đúng cách.
- Hộp nhựa, hoặc giá đựng: chứa tuýp bệnh phẩm.
Mẫu bệnh phẩm hô hấp và mẫu máu của cùng một NB được để trong một hộp nhựa có nắp vặn kín hoặc giá nhựa đựng tuýp bệnh phẩm.
- Thùng vận chuyển mẫu: chứa hộp (hoặc giá) đựng mẫu bệnh phẩm.
+ Thùng chắc chắn, có nắp đậy kín, đảm bảo không vỡ.
+ Có khả năng giữ nhiệt (sử dụng bình tích lạnh)
- Các bước đóng gói vận chuyển mẫu bệnh phẩm
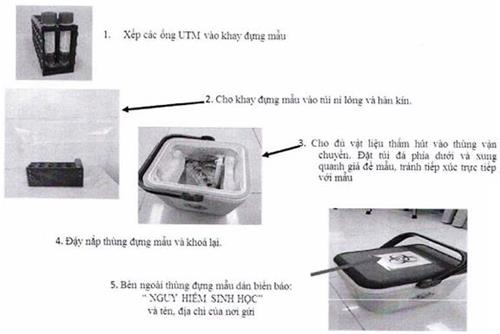
Lưu ý:
- Gửi kèm Phiếu yêu cầu xét nghiệm
- Bên ngoài thùng vận chuyển mẫu có vẽ các logo quy định của WHO (nhãn nguy hại sinh học, nhãn định hướng và nhãn tránh va đập) khi vận chuyển.
Hình 14. Mẫu nhãn biển báo nguy hại sinh học; định hướng; tránh va đập
(Ban hành kèm theo Nghị định số 92/2010/NĐ-CP ngày 30/8/2010 của Chính phủ)
5.5. Quy định về vận chuyển bệnh phẩm
- Thông báo cho phòng xét nghiệm ngày gửi và thời gian dự định bệnh phẩm sẽ tới phòng XN.
- Bệnh phẩm được vận chuyển tới phòng XN bằng đường bộ hoặc đường không càng sớm càng tốt.
- Trong phạm vi bệnh viện, vận chuyển bệnh phẩm bằng tay. Không sử dụng hệ thống vận chuyển bệnh phẩm bằng khí nén.
- Tuyệt đối tránh để tuýp bệnh phẩm bị đỗ, vỡ trong quá trình vận chuyển.
- Bảo đảm tất cả các nhân viên vận chuyển bệnh phẩm được đào tạo về thực hành xử lý an toàn và quy trình khử nhiễm sự cố tràn máu, dịch.
- Nên bảo quản bệnh phẩm ở nhiệt độ 4°C khi vận chuyển tới phòng XN, tránh quá trình đông tan băng nhiều lần, làm giảm chất lượng của bệnh phẩm.
- Bệnh phẩm cần gửi kèm với Phiếu yêu cầu xét nghiệm có đầy đủ thông tin theo quy định.
6. Kiểm tra, giám sát
- Khoa KSNK, phòng Điều dưỡng, Trưởng khoa và Điều dưỡng trưởng các khoa liên quan có nhiệm vụ huấn luyện, kiểm tra giám sát và đôn đốc việc thực hiện nghiêm ngặt quy trình, quy định về an toàn sinh học, sử dụng phương tiện PHCN thành thạo trong quá trình lấy, bảo quản, đóng gói và vận chuyển, xử lý và làm các XN liên quan đến bệnh phẩm COVID-19.
- Giám sát xử lý chất thải y tế có nguy cơ lây nhiễm cao đối với dụng cụ lấy bệnh phẩm, dụng cụ XN và bệnh phẩm thừa sau khi làm XN.
- Giám sát xử lý khu vực lấy bệnh phẩm, xử lý và làm các XN liên quan đến COVID-19.
Xem thêm Hướng dẫn chẩn đoán, điều trị bệnh viêm phổi cấp do chủng vi rút Corona mới (nCoV) ban hành theo Quyết định số 125/QĐ-BYT ngày 16/01/2020 và Hướng dẫn tạm thời giám sát và phòng, chống bệnh viêm đường hô hấp cấp do chủng mới của vi rút Corona (nCoV) ban hành theo Quyết định số 343/QĐ-BYT ngày 07/02/2020 của Bộ trưởng Bộ Y tế.
PHÒNG NGỪA LÂY NHIỄM COVID-19 TRONG XÉT NGHIỆM
1. Mục đích
- Phòng ngừa lây nhiễm COVID-19 qua đường giọt bắn và qua đường tiếp xúc từ các loại bệnh phẩm và những người tiếp xúc với NB trong quá trình làm các XN bệnh phẩm của người nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Tất cả nhân viên trong phòng XN đều phải thực hiện đúng và nghiêm ngặt quy trình và quy định khi lấy mẫu, bảo quản và vận chuyển mẫu.
- Tránh phát tán nguồn bệnh, bảo đảm an toàn cho NVYT và môi trường.
2. Đối tượng áp dụng
- Nhân viên phòng XN tuân thủ nghiêm ngặt các quy định về an toàn sinh học, phải sử dụng thành thạo phương tiện PHCN.
- Tất cả bệnh phẩm của người nhiễm hoặc nghi ngờ nhiễm COVID-19 có thể từ khoa khám bệnh; cấp cứu; truyền nhiễm... hoặc từ cơ sở KBCB khác chuyển đến.
3. Phương pháp áp dụng
3.1. Bệnh phẩm
- Bệnh phẩm đường hô hấp trên.
- Bệnh phẩm đường hô hấp dưới.
- Mẫu huyết thanh
3.2. Xét nghiệm các ca bệnh nghi ngờ
- Xét nghiệm huyết học.
- Xét nghiệm hóa sinh.
- Xét nghiệm vi sinh.
+ Chẩn đoán phân biệt:
• Cúm nặng.
• Viêm phổi không điển hình.
• Nhiễm khuẩn huyết gây suy thận và suy hô hấp.
• Bệnh tay chân miệng thể cấp có biến chứng suy hô hấp và suy thận.
+ Các xét nghiệm thường quy khác.
3.3. Xét nghiệm xác định COVID-19
Phát hiện COVID-19 dương tính bằng kỹ thuật Real time RT-PCR hoặc giải trình tự gen thế hệ mới.
4. Yêu cầu đảm bảo an toàn sinh học
Phòng ngừa lây nhiễm COVID-19 qua đường giọt bắn, đường tiếp xúc và đường phát tán khí dung khi thực hiện thao tác tạo khí dung là ưu tiên hàng đầu trong quá trình làm XN cho người nghi ngờ nhiễm hoặc nhiễm COVID-19.
4.1. Cơ sở vật chất
- Các XN thường quy: An toàn sinh học cấp II
- Các XN chẩn đoán COVID-19: An toàn sinh học cấp II
4.2. Trang thiết bị
- Đảm bảo các yêu cầu về trang thiết bị đối với phòng XN An toàn sinh học cấp II.
- Tủ An toàn sinh học cấp II đã được hiệu chuẩn, chứng nhận.
- Phương tiện PHCN:
+ Các XN thường quy: Phương tiện PHCN thông thường.
+ Các XN chẩn đoán xác định COVID-19: đầy đủ phương tiện PHCN, bao gồm: Bộ quần áo chống dịch, găng tay không bột, khẩu trang N95, kính bảo hộ hoặc tấm che mặt.
4.3. Nhân viên xét nghiệm
- Nhân viên phòng XN khi tiến hành các XN cho người nhiễm hoặc nghi ngờ nhiễm COVID-19 phải có kinh nghiệm, thành thạo, Nên bố trí nhân viên chuyên biệt làm các XN này.
- Tuân thủ nghiêm ngặt các quy định về an toàn sinh học, sử dụng phương tiện PHCN thành thạo, đúng quy cách.
- Khi thực hiện XN thường quy: phải mặc phương tiện PHCN thông thường như đeo găng tay, áo chống thấm nước, tấm che mặt hoặc kính bảo hộ, khẩu trang.
- Khi thực hiện xét nghiệm chẩn đoán xác định COVID-19 phải mặc đầy đủ phương tiện PHCN, bao gồm cả găng tay, quần áo chống dịch, khẩu trang chuyên dụng (N95), tấm che mặt hoặc kính bảo hộ.
- Trong khi đeo găng tay làm XN liên quan đến bệnh phẩm người nghi ngờ hoặc người xác định nhiễm COVID-19 không được đụng chạm lên bàn phím điều khiển máy móc thiết bị, nắm cửa, điện thoại, công tắc điện...
- Người thực hiện các XN cho người nhiễm hoặc nghi ngờ nhiễm COVID-19 không được mặc phương tiện PHCN khi ra ngoài phòng xét nghiệm COVID-19.
- Hiểu được nguy cơ nhiễm bệnh, có khả năng phát hiện và đánh giá nguy cơ cho cá nhân, có kiến thức kiểm soát sức khoẻ sau khi làm nhiệm vụ và tự xử lý theo đúng quy trình khi bị phơi nhiễm.
- Tuyệt đối không tiếp xúc tay trần với bệnh phẩm và dụng cụ làm XN cho người nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Khi thực hiện các XN liên quan đến bệnh phẩm của NB dương tính (+) với COVID-19 hay nghi ngờ cẩn thận trọng không đụng tay lên vùng mặt, mũi, miệng.
5. Kiểm tra, giám sát
Khoa KSNK, Phòng Điều dưỡng, Trưởng khoa và Điều dưỡng trưởng các khoa liên quan có nhiệm vụ huấn luyện, kiểm tra giám sát và đôn đốc việc thực hiện nghiêm ngặt quy trình, quy định an toàn sinh học khi thực hiện XN NB nghi ngờ hoặc nhiễm COVID-19.
- Giám sát NVYT việc tuân thủ nghiêm ngặt khử khuẩn dụng cụ và khu vực lấy bệnh phẩm.
- Giám sát NVYT việc tuân thủ nghiêm ngặt các quy định về an toàn sinh học, sử dụng phương PHCN thành thạo trong quá trình XN.
- Giám sát xử lý dụng cụ tái sử dụng sau khi làm XN.
- Giám sát xử lý chất thải y tế có nguy cơ lây nhiễm cao đối với bệnh phẩm sau khi làm XN.
- Giám sát xử lý môi trường buồng xét nghiệm như khu vực cách ly.
Lưu ý:
- Khu vực lấy mẫu phải được xử lý như khu vực cách ly.
- Phòng XN đảm bảo thông khí, không thải khí ra nơi có nhiều người qua lại, vào hành lang hoặc các phòng khác.
- Các thao tác xét nghiệm có nguy cơ tạo khí dung, giọt bắn cần được thực hiện trong tủ an toàn sinh học cấp II như mở nắp ống nghiệm chứa mẫu bệnh phẩm; phân chia, pha loãng mẫu bệnh phẩm; trộn mẫu (vortex); tách chiết DNA/RNA.
- Tay đi găng làm XN liên quan đến bệnh phẩm người bệnh COVID-19 không được đụng chạm lên bàn phím điều khiển máy móc thiết bị, nắm cửa, điện thoại, công tắc điện...
- Tất cả trang phục phòng hộ (găng, áo choàng, khẩu trang...) khi cởi bỏ phải cuộn mặt bẩn (mặt bên ngoài) vào trong để hạn chế nguy cơ phát tán tác nhân lây nhiễm ra các vật dụng thu gom, vận chuyển.
- Dụng cụ lấy bệnh phẩm và bệnh phẩm của người nhiễm hoặc nghi ngờ nhiễm COVID-19 sau khi làm xong XN phải được xử lý như chất thải y tế có nguy cơ lây nhiễm cao.
XỬ LÝ THI HÀI NGƯỜI NHIỄM HOẶC NGHI NGỜ NHIỄM COVID-19
1. Mục đích
- Nhân viên y tế xử lý đúng và nghiêm ngặt quy trình, quy định khi xử lý thi hài nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Phòng ngừa lây nhiễm COVID-19 cho NVYT và người nhà NB, người tham dự tang lễ và cộng đồng.
2. Phạm vi áp dụng
- Khoa Giải phẫu bệnh, nhà đại thể và các khoa lâm sàng có người nhiễm hoặc nghi ngờ nhiễm COVID-19 tử vong.
- Nhân viên y tế và người nhà NB trực tiếp có tiếp xúc với thi hài người nhiễm hoặc nghi ngờ nhiễm COVID-19.
3. Nguyên tắc chung
- Áp dụng triệt để các biện pháp phòng ngừa chuẩn và phòng ngừa cách ly theo đường tiếp xúc và giọt bắn khi vận chuyển, xử lý thi hài.
- Chỉ NVYT có nhiệm vụ, người nhà NB đã được hướng dẫn quy trình phòng ngừa và được trang bị đầy đủ phương tiện PHCN phù hợp mới được tham gia xử lý thi hài người nhiễm hoặc nghi ngờ nhiễm COVID-19 tử vong.
- Đảm bảo không phát tán mầm bệnh trong quá trình xử lý, vận chuyển, hỏa táng và mai táng thi hài người nhiễm hoặc nghi ngờ nhiễm COVID-19 tử vong.
- Chuyển NB cách ly khác trong buồng bệnh (nếu có) sang buồng cách ly khác trước khi thực hiện xử lý thi hài.
- Thi hài người nhiễm hoặc nghi ngờ nhiễm COVID-19 phải được hỏa táng, chỉ mai táng trong trường hợp không thực hiện được việc hỏa táng.
- Thi hài phải được khâm liệm càng sớm càng tốt và hỏa táng hoặc mai táng trong vòng 24 giờ kể từ khi tử vong.
- Tất cả các chất thải phát sinh trong quá trình xử lý, vận chuyển, hỏa táng hoặc mai táng thi hài người nhiễm hoặc nghi ngờ nhiễm COVID-19 phải được xử lý như chất thải lây nhiễm.
4. Phương tiện
4.1. Phương tiện vận chuyển, bảo quản và xử lý thi hài
- Xe, cáng vận chuyển thi hài phải được vệ sinh khử khuẩn ngay sau mỗi lần sử dụng.
- Túi chuyên dụng đựng tử thi, trường hợp không có thì phải có túi nilon không thấm nước có khóa kéo, bảo đảm độ bền cơ học, kích thước phù hợp và ga giường sử dụng một lần.
- Buồng lạnh bảo quản thi hài hoặc buồng giữ thi hài được trang bị phương tiện rửa tay, hoá chất khử khuẩn bề mặt, sàn nhà và các phương tiện vệ sinh khử khuẩn bề mặt.
4.2. Phương tiện phòng hộ cá nhân, vệ sinh tay và thu gom chất thải
Tại khoa lâm sàng có người nhiễm hoặc nghi ngờ nhiễm COVID-19 và tại nhà đại thể cần luôn có sẵn các phương tiện cho thực hành phòng ngừa lây nhiễm, gồm:
- Phương tiện VST: xà phòng rửa tay, dung dịch VST chứa cồn.
- Phương tiện PHCN: là các phương tiện sử dụng một lần (găng tay, mũ giấy, khẩu trang y tế, áo choàng, kính bảo hộ, tạp dề). Các phương tiện này phải là loại không thấm nước.
- Phương tiện thu gom chất thải: túi, thùng màu vàng có kích thước đủ lớn để thu gom các phương tiện PHCN sau sử dụng.
- Hóa chất khử khuẩn tử thi: dung dịch có Clo hoạt tính 0,5%.
- Phương tiện vệ sinh, khử khuẩn môi trường: Khăn lau, tải lau bề mặt, bình phun tay hoặc máy phun tay.
5. Biện pháp tiến hành
5.1. Tại đơn vị có người nhiễm hoặc nghi ngờ nhiễm COVID-19 tử vong
Ngay khi có người nhiễm hoặc nghi ngờ nhiễm COVID-19 tử vong, NVYT trực tiếp điều trị, chăm sóc NB cần thực hiện các nội dung sau:
- Không bố trí NB khác (kể cả người nhiễm hoặc nghi ngờ nhiễm COVID-19) trong buồng bệnh đang có thi hài. Trường hợp trong buồng bệnh có NB khác thì phải chuyển ngay NB đó sang buồng bệnh khác.
- Gọi điện thoại thông báo và viết giấy yêu cầu nhà đại thể cử nhân viên chuyển tử thi về nhà đại thể.
- Nghiêm cấm người không có nhiệm vụ và người nhà NB vào buồng bệnh.
- Giải thích cho người nhà NB về nguy cơ lây nhiễm và hướng dẫn họ các quy định và biện pháp phòng ngừa lây nhiễm cần áp dụng khi tiếp xúc với tử thi và trong quá trình khâm liệm, thăm viếng.
- Tuyệt đối không mang bất cứ vật dụng gì ra khỏi buồng bệnh khi buồng bệnh chưa được phun khử khuẩn lần cuối.
- Trong khi chờ nhân viên đại thể đến lấy xác, nhân viên khoa phòng che phủ tử thi băng ga trải giường, lau bề mặt toàn bộ khu vực NB nằm bằng dung dịch Clo hoạt tính 0,5%.
- Nhân viên nhà đại thể mặc đầy đủ phương tiện PHCN khi thực hiện xử lý thi hài. Chi tiết phương tiện PHCN cho nhân viên xử lý thi hài tại Phụ lục 3.
- Tiến hành cô lập tử thi theo các bước sau:
+ Bọc kín tử thi bằng túi đựng thi hài, sử dụng vật liệu chống thấm lót bên trong nếu có nguy cơ thấm dịch tiết ra ngoài.
+ Phun khử khuẩn bên ngoài lớp túi thứ nhất bằng dung dịch hóa chất khử trùng có Clo với nồng độ 0,5% (5.000 ppm) Clo hoạt tính. Thực hiện tương tự với lớp túi đựng tử thi thứ hai. Túi đựng tử thi phải bằng vật liệu chống thấm, không trong suốt, chắc chắn, không dễ bị bục/thủng, thành túi có độ dày ≥ 150μm; Khóa kéo phải kín và chắc chắn.
+ Trường hợp không có túi đựng tử thi, bọc kín tử thi bằng 02 lớp vải cotton dày, sau đó bọc kín tử thi bằng 02 lớp ni-lon. Phun khử khuẩn bên ngoài lớp ni-lon thứ nhất bằng dung dịch hóa chất khử trùng có Clo với nồng độ 0,5% (5.000ppm) Clo hoạt tính. Thực hiện tương tự với lớp ni-lon thứ hai.
+ Sau khi đóng kín túi đựng tử thi, sử dụng thẻ hoặc miếng dán có biểu tượng nguy hại sinh học (theo mẫu trong Quy chế quản lý chất thải y tế, ban hành kèm theo Quyết định 43/2007/QĐ-BYT) ở bên ngoài túi.
+ Trải một chiếc vải trải giường sạch lên xe chở tử thi, đặt tử thi lên trên tấm vải sạch, đi tới gần cửa buồng bệnh và tháo bỏ phương tiện PHCN (để đồ tháo bỏ ở phía trong buồng bệnh), khử khuẩn tay và ra ngoài buồng bệnh.
+ Nhân viên nhà đại thể mang đủ phương tiện PHCN tiếp nhận thi hài bên ngoài buồng bệnh, vận chuyển tử thi về nhà đại thể.
- Khử khuẩn lại toàn bộ buồng bệnh, hành lang sau khi xử lý.
- Trong suốt thời gian kể từ khi NB tử vong tới khi mang tử thi ra khỏi buồng bệnh, NVYT tại khoa có NB tử vong cần giám sát nhắc nhở tất cả đối tượng vào buồng bệnh phải thực hiện đúng quy định về cách ly phòng ngừa lây nhiễm.
5.2. Vận chuyển tử thi từ buồng bệnh về nhà đại thể
- Nhân viên y tế trong suốt quá trình vận chuyển tử thi phải mang đầy đủ phương tiện PHCN (khẩu trang ngoại khoa, găng tay, áo choàng giấy, mũ, ủng). Chi tiết phương tiện PHCN cho nhân viên xử lý thi hài tại Phụ lục 3.
- Vận chuyển tử thi theo đường cách ly và phải phun khử khuẩn ngay sau đó; Nếu vận chuyển bằng thang máy thì không cho người khác đi cùng, trong trường hợp người nhà NB yêu cầu đi cùng thì phải mang đầy đủ phương tiện PHCN. Hạn chế vận chuyển tử thi qua nơi đông người.
- Ngay sau khi đưa tử thi vào phòng lưu giữ, nhân viên nhà đại thể vận chuyển tử thi phải tiến hành phun khử khuẩn xe vận chuyển tử thi bằng dung dịch có nồng độ 0,05% (500 ppm) Clo hoạt tính để trong vòng 30 phút, sau đó tháo bỏ phương tiện PHCN theo đúng trình tự, thải bỏ các phương tiện này vào túi nilon màu vàng, rửa sạch tay và vệ sinh cá nhân trước khi thực hiện các nhiệm vụ khác.
5.3. Khâm liệm tử thi
Quá trình khâm liệm tuân theo quy trình đặc biệt đối với bệnh dịch nguy hiểm:
- Thực hiện khâm liệm càng sớm càng tốt.
- Khâm liệm tử thi phải được thực hiện tại nhà tang lễ bệnh viện. Hạn chế tối đa số người tham gia khâm liệm.
- Người trực tiếp tham gia khâm liệm phải mang đầy đủ phương tiện PHCN (khẩu trang ngoại khoa, găng tay, áo choàng giấy, mũ, ủng). Vệ sinh tay bằng dung dịch chứa cồn và rửa sạch tay bằng xà phòng.
- Tuyệt đối không để người nhà NB thăm viếng tử thi trong suốt thời gian lưu giữ cho tới khi khâm liệm xong.
- Quy trình khâm liệm tử thi:
+ Lót một tấm vải ni-lon lớn đủ để bao bọc tử thi dưới đáy quan tài.
+ Gói kín thi hài bằng tấm vải ni-lon đã lót phía dưới.
+ Đóng kín quan tài. Kiểm tra và dán kín các kẽ hở của quan tài (nếu có) bằng băng dính không thấm nước.
- Nhân viên nhà tang lễ thực hiện phun khử khuẩn toàn bộ bề mặt buồng khâm liệm và bề mặt quan tài bằng dung dịch chứa 0,05% Clo hoạt tính.
+ Tháo các phương tiện PHCN (khẩu trang ngoại khoa, găng tay, áo choàng giấy, mũ, ủng) và thải bỏ vào túi nilon màu vàng.
+ Vệ sinh tay bằng dung dịch chứa cồn và rửa sạch tay bằng xà phòng.
+ Tắm vệ sinh thân thể trước khi thực hiện các nhiệm vụ khác.
5.4. Thăm viếng, xử lý tử thi người nhiễm hoặc nghi ngờ nhiễm COVID-19
- Hạn chế người vào viếng. Người vào viếng phải mang khẩu trang, không đụng chạm vào quan tài và VST bằng dung dịch cồn sau khi viếng.
- Không vận chuyển thi hài ra ngoại tỉnh. Chuyển thi hài bằng xe ô tô chuyên dụng thẳng tới nơi hoả táng. Người nhà NB không được lên xe chuyển thi hài. Nhân viên lái xe chuyển thi hài phải mang đầy đủ phương tiện PHCN.
- Thi hài người nhiễm hoặc nghi ngờ nhiễm COVID-19 cần được hỏa táng càng sớm càng tốt, không để quá 24 giờ kể từ khi tử vong.
- Ngay sau khi vận chuyển quan tài tới nơi hỏa táng, mai táng phải khử khuẩn toàn bộ bề mặt phương tiện chở quan tài bằng dung dịch khử khuẩn đã được Bộ Y tế cấp chứng nhận đăng ký lưu hành.
- Trường hợp có nhu cầu vận chuyển thi hài, hài cốt qua biên giới thực hiện theo quy định tại Nghị định số 89/2018/NĐ-CP ngày 25/6/2018 của Chính phủ quy định chi tiết thi hành một số điều của Luật Phòng, chống bệnh truyền nhiễm về kiểm dịch y tế biên giới.
6. Kiểm tra giám sát và trách nhiệm
- Khoa KSNK, Phòng Điều dưỡng, Trưởng khoa và Điều dưỡng trưởng các khoa liên quan có nhiệm vụ huấn luyện, kiểm tra giám sát và đôn đốc việc thực hiện nghiêm ngặt quy trình, quy định xử lý thi hài người nghi ngờ nhiễm hoặc nhiễm COVID-19:
- Đơn vị có NB tử vong: đảm bảo tuân thủ các quy định phòng chống lây nhiễm tại khu vực mình quản lý.
- Nhà tang lễ: thực hiện nhận thi hài, vận chuyển tử thi xuống nhà đại thể, khâm liệm tử thi và tổ chức thăm viếng, xử lý thi hài theo quy định.
- Đơn vị dịch vụ: bố trí xe vận chuyển tử thi và thực hiện các quy định trong quá trình vận chuyển thi hài tới nghĩa trang. Chuẩn bị sẵn một cơ số phương tiện PHCN để nhượng lại cho người nhà NB sử dụng khi cần.
- Phòng Kế hoạch tổng hợp: giám sát thực hiện, tiếp nhận và báo cáo xin ý kiến Ban chỉ đạo bệnh viện giải quyết các vướng mắc nảy sinh trong quá trình thực hiện quy định này.
- Khoa KSNK: tổ chức kiểm tra, giám sát việc thực hiện theo đúng quy định.
- Lập danh sách tất cả NVYT, người nhà... có tham gia xử lý và khâm niệm tử thi để báo cáo và theo dõi trong 14 ngày theo quy định đồng thời hướng dẫn họ các triệu chứng cần phát hiện, báo cáo và đi khám.
HƯỚNG DẪN PHÒNG NGỪA LÂY NHIỄM COVID-19 CHO NGƯỜI NHÀ VÀ KHÁCH THĂM
Người nhà và khách thăm là đối tượng có nguy cơ bị lây nhiễm và phát tán nguồn lây ra cộng đồng cao. Tất cả các cơ sở y tế phải xây dựng, tuyên truyền hạn chế tối đa thăm và phải cung cấp phương tiện PHCN cho các đối tượng này.
1. Mục đích
- Phòng ngừa lây nhiễm cho khách thăm, người nhà NB của NB khi phải tiếp xúc với người nhiễm hoặc nghi ngờ nhiễm COVID-19.
- Bảo đảm an toàn cho cộng đồng, tránh lây lan COVID-19 trên diện rộng.
2. Nguyên tắc thực hiện
- Tuyệt đối không để người tiếp xúc gần, thăm viếng khi người nhiễm hoặc nghi ngờ nhiễm đang cách ly điều trị, theo dõi tại cơ sở KBCB.
- Không cho khách thăm tại khu vực cách ly khi đang thực hiện các thủ thuật có thể tạo khí dung, các hạt văng bắn gần để phòng lây nhiễm nguy hiểm.
- Hạn chế tối đa việc thăm viếng của khách tới khu vực cách ly đề phòng lây lan dịch bệnh ra cộng đồng.
- Trong trường hợp bắt buộc phải có thăm, tiếp xúc với NB tất cả khách thăm cần tuân thủ nguyên tắc phòng ngừa tại khu cách ly. Khách thăm được hướng dẫn biết cách mang, loại bỏ phương tiện PHCN trước khi đến khu vực cách ly thăm.
- Khi được phép thăm, không cho khách thăm tiếp xúc gần với NB (trong phạm vi 2 mét).
- Những bà mẹ khi nghi ngờ nhiễm hoặc đã xác định nhiễm COVID-19 đang cho con bú phải cách ly con tránh lây lan và không cho trẻ dùng sữa mẹ cho đến khi có chỉ định của bác sĩ điều trị.
Khi ra khỏi khu vực cách ly sau khi thăm viếng phải tuân thủ quy trình loại bỏ phương tiện PHCN và VST đúng quy định trước khi rời khỏi khu cách ly. Cung cấp đầy đủ thông tin cá nhân và giữ liên lạc thường xuyên với cơ quan y tế theo hướng dẫn để theo dõi phơi nhiễm sau tiếp xúc.
- Cần có NVYT đi kèm và hướng dẫn khách thăm tuân thủ nghiêm ngặt và ghi tên lại để tiếp tục theo dõi.
3. Đối tượng và phạm vi áp dụng: Tất cả khách thăm, người nhà NB, NVYT có tiếp xúc gần với NB tại mọi thời điểm cách ly.
4. Thực hiện
4.1. Trước khi vào buồng cách ly
- Người nhà NB và khách thăm trước khi vào khu vực cách ly phải được hướng dẫn và mang phương tiện PHCN đúng quy định, đặc biệt lưu ý với những phương tiện PHCN phòng ngừa lây truyền qua đường hô hấp.
- Nhân viên y tế có mặt để hướng dẫn khách thăm thực hiện đúng các bước; mang và loại bỏ phương tiện PHCN và giám sát hành động của khách thăm.
- Nhân viên y tế kiểm tra tuân thủ đúng hướng dẫn và hiểu rõ các yêu cầu phòng ngừa lây nhiễm mới được cho phép vào khu cách ly thăm.
4.2. Trong phòng cách ly
- Tất cả khách thăm phải tuân thủ đúng hướng dẫn và giám sát của NVYT tại khu cách ly, không được tùy tiện đụng chạm đến tất cả tất cả vật dụng trong khu cách ly, không tiếp xúc trực tiếp với NB (ôm hôn, bắt tay).
- Giữ khoảng cách tối thiểu 2 mét so với người bệnh.
4.3. Ra khỏi phòng cách ly
- Tháo bỏ trang phục phòng hộ theo hướng dẫn của NVYT ngay tại vùng đệm khu cách ly.
- Không mang theo bất cứ vật dụng, trang phục PHCN tại khu cách ly sau khi sử dụng đến nơi khác.
- Lập danh sách những người có tiếp xúc gần với người nhiễm và nghi ngờ nhiễm COVID-19 và thông báo với cơ quan y tế dự phòng địa phương để theo dõi tình hình sức khỏe và xử lý theo quy định.
- Tư vấn cho người nhà và khách thăm chủ động khai báo đầy đủ các thông tin cá nhân liên quan để theo dõi và tự theo dõi các triệu chứng sau khi rời khỏi khu cách ly trong vòng 14 ngày. Khi có biểu hiện bất thường về sức khoẻ phải đến ngay cơ quan y tế gần nhất báo cáo để được tư vấn.
- Kiểm tra giám sát:
+ Khoa KSNK, Phòng Điều dưỡng, Trưởng khoa và Điều dưỡng trưởng các khoa liên quan có nhiệm vụ huấn luyện, kiểm tra giám sát và đôn đốc việc thực hiện nghiêm ngặt quy trình, quy định tham gia vào quá trình chăm sóc NB hoặc thăm viếng người nghi ngờ hoặc nhiễm COVID-19 bao gồm:
+ Giám sát việc NVYT có huấn luyện, hướng dẫn, giám sát người nhà, khách thăm hay không.
PHỤ LỤC
PHỤ LỤC 1
SƠ ĐỒ TIẾP NHẬN NGƯỜI BỆNH NGHI NGỜ NHIỄM COVID-19
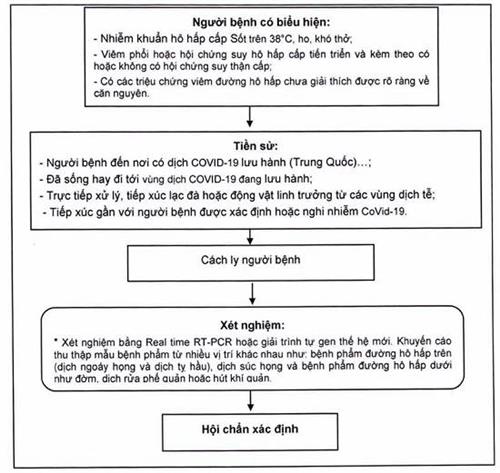
PHỤ LỤC 2
SƠ ĐỒ THỰC HIỆN PHÒNG NGỪA VÀ KIỂM SOÁT NHIỄM KHUẨN THEO TỪNG GIAI ĐOẠN CHẨN ĐOÁN
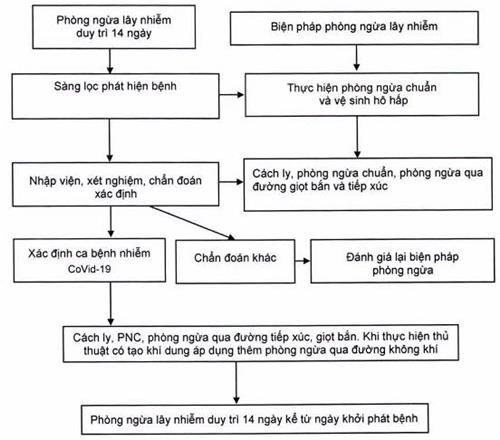
PHỤ LỤC 3
SỬ DỤNG PHƯƠNG TIỆN PHÒNG HỘ CÁ NHÂN CỦA NHÂN VIÊN Y TẾ TRONG PHÒNG CHỐNG COVID-19
|
Vị trí, thủ thuật |
Sử dụng phương tiện phòng hộ cá nhân |
|||||
|
Bộ quần áo chống dịch |
Tạp dề |
Găng |
Khẩu trang y tế |
Khẩu trang N95 |
Kính bảo hộ / tấm che mặt |
|
|
Tiếp đón |
|
|
+/- |
+ |
|
|
|
Phòng khám sàng lọc |
+ |
|
+ |
+ |
+/- |
+ |
|
Khu vực cách li trong BV |
+ |
+/- |
+ |
|
+ |
+ |
|
Phòng xét nghiệm |
+ |
+/- |
+ |
|
+ |
+ |
|
Vận chuyển người bệnh |
+ |
+/- |
+ |
+ |
+/- |
+ |
|
Khu xử lý, bảo quản thi hài |
+ |
+/- |
+ |
+ |
+/- |
+ |
Ghi chú: (+) Cần thiết sử dụng.
(+/-) Cân nhắc sử dụng theo từng trường hợp.
PHỤ LỤC 4
CÁC HÓA CHẤT SỬ DỤNG TRONG PHÒNG CHỐNG DỊCH
Bệnh dịch ngày càng có xu hướng diễn biến khó lường, tại nhiều nước trên thế giới đang có tình trạng phát sinh, gia tăng những bệnh dịch mới nổi và nguy hiểm. Trong các đợt bùng phát bệnh dịch, việc sử dụng hóa chất để khử trùng các vật dụng và khu vực bị ô nhiễm là rất quan trọng, có thể ngăn chặn dịch lây lan và giảm số nạn nhân.
Có nhiều loại hóa chất khử trùng được sử dụng trong các cơ sở y tế, người sử dụng phải được cung cấp đầy đủ thông tin về những hóa chất đó, các hóa chất phải đảm bảo đạt hiệu quả cao trong các khâu xử lý môi trường, không khí phòng, các thiết bị y tế và chất thải. Dưới đây là một số hóa chất thường dùng để phòng chống bệnh dịch trong các cơ sở y tế hiện nay:
1. Nhóm hóa chất thường dùng để khử khuẩn da và vệ sinh tay
1.1. Cồn (Alcohol)
1.1.1. Đặc điểm chung
Trong khử khuẩn, cồn được sử dụng là cồn Ethyl 70° hoặc cồn Isopropyl 50°. Hiệu quả sát khuẩn của cồn thường được đánh giá cao. Trong các chế phẩm VST, cồn ở mức 60%-80%. Cồn cao độ hơn, bay hơi nhanh nên cũng giảm phần nào hiệu quả sát trùng.
1.1.2. Cơ chế tác dụng
Cồn làm biến tính protein của vi khuẩn, vi rút có tác dụng trên các tế bào sinh dưỡng (kể cả BK- trực khuẩn lao, vi rút có vỏ, nấm) nhưng không có tác dụng trên bào tử.
Cồn phá hủy các cấu trúc lipid của vi rút nên vi rút sẽ bị tiêu diệt trong vài chục giây sau tiếp xúc.
1.1.3. Hướng dẫn sử dụng
Cồn và các chế phẩm của cồn được dung để VST trong quá trình mang và tháo phương tiện PHCN. Ngoài ra cồn còn được dùng để khử khuẩn các dụng cụ như nhiệt kế, dụng cụ nội soi võng mạc, nắp cao su của những lọ thuốc chia nhiều liều hoặc các chai đựng vắc xin, bóng ambu, dụng cụ siêu âm hoặc các dụng cụ sử dụng để pha chế thuốc.
Cồn là chất dễ cháy nên cần lưu giữ trong môi trường mát, điều kiện thông khí tốt. Cồn bốc hơi nhanh do vậy các dụng cụ chứa cồn phải có nắp đậy, các dụng cụ cần khử khuẩn phải được ngâm ngập trong cồn.
1.2. Dung dịch có chứa Chlorhexidinegluconat
1.2.1. Đặc điểm chung
Các dung dịch chứa Chlorhexidine có tác dụng diệt khuẩn nhanh, mạnh, phổ rộng, trong thành phần có bổ sung chất làm mềm, làm ẩm dưỡng da. Tác dụng diệt khuẩn kéo dài hơn so với các các dung dịch chứa cồn và Iodophor, không gây kích ứng da.
1.2.2. Cơ chế tác dụng
Chlorhexidine có hiệu quả trên phạm vi rộng đối với các vi khuẩn Gram (+) và Gram (-), men, nấm da và các vi rút ưa lipid. Thuốc không có tác dụng trên các bào tử.
1.2.3. Hướng dẫn sử dụng
Dung dịch Chlorhexidine 2% sử dụng để khử khuẩn da như tắm, VST, khử khuẩn niêm mạc như khí dung vào miệng.
Dung dịch Chlorhexidine 4% sử dụng để VST trước phẫu thuật, đỡ đẻ.
1.3. Hợp chất Iodophor
1.3.1. Đặc điểm chung
Chất khử khuẩn thuộc nhóm Iodophor được sử dụng trong các cơ sở y tế như Povidone-Iodine (kết hợp giữa Polyvinylpyroiodine và lode) có khả năng diệt vi khuẩn và vi rút nhưng không diệt được bào tử, chất này ít gây kích ứng da và không để lại màu sau khi sử dụng.
1.3.2. Cơ chế tác dụng
Hợp chất Iodophor có khả năng xâm nhập rất nhanh vào vách tế bào của VSV và phá vỡ cấu trúc protein và acid nucleic của chúng.
1.3.3. Hướng dẫn sử dụng
Các hóa chất thuộc nhóm Iodophor được sử dụng trong sát khuẩn da, thay băng vết mổ và khử khuẩn các loại dụng cụ, vật dụng y tế không xâm nhập như nhiệt kế, ống nghe, huyết áp kế...
2. Nhóm hóa chất thường sử dụng trong xử lý môi trường
2.1. Chlorine và hợp chất Chlorine
2.1.1. Đặc điểm chung
Chlorine và các hợp chất chlorin được sử dụng phổ biến nhất trong phòng chống dịch tại các cơ sở y tế. Loại hóa chất này tồn tại dưới hai dạng: dạng lỏng (Javel) hoặc dạng ran (Calcium Hypochloride). Các chất khử khuẩn chlorine có phổ kháng khuẩn rộng, diệt vi khuẩn nhanh, giá thành thấp. Tuy nhiên, hạn chế của loại hóa chất này là ăn mòn các dụng cụ, vật dụng y tế khi tiếp xúc và hoạt tính giảm khi có mặt các chất hữu cơ.
Những hợp chất giải phóng Chlorine được sử dụng trong bệnh viện bao gồm hai loại: Cloramin B (Dioxide Chlorine) và Cloramin T.
2.1.2. Cơ chế tác dụng
Sự có mặt của hợp chất Chlorine làm ức chế các phản ứng của những enzyme cần thiết tham gia vào quá trình nhân lên của vi rút, làm thay đổi bản chất protein và bất hoạt các acid nucleic của vi rút.
2.2.3. Hướng dẫn sử dụng
Các dung dịch khử khuẩn có Chlorine cần đạt nồng độ tối thiểu 0,05% (500 ppm) sau khi pha. Dung dịch pha 0,05% được sử dụng để khử nhiễm các bề mặt như sàn nhà, tường, trần nhà... Với các phương tiện vận chuyển như xe cứu thương, cáng, vật dụng khác phải được phun khử khuẩn sau khi vận chuyển.
Các dung dịch pha từ các hóa chất chứa Clo trên thị trường hiện nay với nồng độ 0,05, 0,5%, 1% và 1,25% Clo hoạt tính thường được sử dụng tùy theo mục đích và cách thức của việc khử khuẩn. Việc tính nồng độ dung dịch phải dựa vào clo hoạt tính. Vì các hóa chất khác nhau có hàm lượng clo hoạt tính khác nhau, cho nên phải tính toán đủ khối lượng hóa chất cần thiết để đạt được dung dịch có nồng độ clo hoạt tính muốn sử dụng.
Lượng hóa chất chứa Clo cần để pha số lít dung dịch với nồng độ Clo hoạt tính theo yêu cầu được tính theo công thức sau:
|
Lượng hóa chất (gam) |
= |
Nồng độ clo hoạt tính của dung dịch cần pha (%) x số lít |
x |
1.000 |
|
Hàm lượng clo hoạt tính của hóa chất sử dụng (%) |
* Hàm lượng Clo hoạt tính của hóa chất sử dụng luôn được nhà sản xuất ghi trên nhãn, bao bì hoặc bảng hướng dẫn sử dụng sản phẩm.
Ví dụ:
- Để pha 10 lít dung dịch có nồng độ clo hoạt tính 0,5% từ bột Cloramin B 25% Clo hoạt tính, cần: (0,5 x 10/25) x 1.000 = 200 gam.
- Để pha 10 lít dung dịch có nồng độ clo hoạt tính 0,5% từ bột Canxi hypocloride 70% Clo hoạt tính, cần: (0,5 x 10/70 ) x 1.000 = 72 gam.
- Để pha 10 lít dung dịch có nồng độ clo hoạt tính 0,5% từ bột Natri dichloroisocianurate 60% Clo hoạt tính, cần: (0,5 x 10/60) x 1.000 = 84 gam.
Bảng 1. Lượng hóa chất chứa Clo để pha 10 lít dung dịch với các nồng độ Clo hoạt tính thường sử dụng trong vệ sinh bề mặt môi trường trong bệnh viện
|
Tên hóa chất (hàm lượng clo hoạt tính) |
Lượng hóa chất cần để pha 10 lít dung dịch có nồng độ clo hoạt tính |
Cách pha |
||||
|
0,05% |
0,25% |
0,5% |
1,25% |
2,5% |
||
|
Cloramin B 25% |
20g |
100g |
200g |
500g |
1000g |
Hòa tan hoàn toàn lượng hóa chất cần thiết cho vừa đủ với 10 lít nước sạch, ở nhiệt độ thường. |
|
Canxi HypoCloride 70% |
7,2g |
36g |
72g |
180g |
360g |
|
|
Bột Natri Dichloro_ isocyanurate 60% |
8,4g |
42g |
84g |
210g |
420g |
|
Cholorine được sử dụng phổ biến trong khử khuẩn nước. Việc sử dụng chlorine ở nồng độ cao làm giảm đáng kể số lượng vi khuẩn trong các nguồn nước bị ô nhiễm.
Các dung dịch khử trùng có Clo sẽ giảm tác dụng nhanh theo thời gian, cho nên chỉ pha đủ lượng cần sử dụng và phải sử dụng càng sớm càng tốt sau khi pha. Tốt nhất chỉ pha và sử dụng trong ngày, không nên pha sẵn để dự trữ. Dung dịch đã pha cân bảo quản ở nơi khô, mát, đậy kín, tránh ánh sáng.
2.2. Hợp chất ammonium bậc 4
Hợp chất Ammonium bậc 4 được sử dụng như các chất khử khuẩn trong bệnh viện, chúng có khả năng diệt nấm, vi khuẩn, lipophilics vi rút nhưng không có khả năng diệt bào tử. Loại hợp chất này chỉ được sử dụng như hoá chất khử khuẩn mà không được sử dụng với vai trò là chất sát khuẩn đối với da hay các mô của cơ thể.
Những hợp chất Ammonium bậc 4 là các tác nhân làm sạch rất tốt, nhưng với COVID-19 hiệu quả không cao nên không khuyến khích sử dụng.
3. Nhóm hóa chất dùng khử khuẩn, tiệt khuẩn dụng cụ
3.1. Glutaraldehyde
3.1.1.Đặc điểm chung
Bản chất của Glutaraldehyde là các Dialdehyde bão hoà. Glutaraldehyde được sử dụng với vai trò như một hóa chất tiệt khuẩn và khử khuẩn mức độ cao. Dung dịch Glutaraldehyde mang tính acid và không có khả năng diệt bào tử. Chỉ khi dung dịch được hoạt hóa bằng các tác nhân gây kiềm hoá ở pH từ 7,5 - 8,5, lúc này dung dịch mới có khả năng diệt bào tử.
Glutaraldehyde được sử dụng rộng rãi tại các cơ sở y tế bởi những lý do sau:
- Hoạt tính diệt khuẩn tốt;
- Hoạt tính diệt khuẩn không bị thay đổi ngay cả khi có mặt các chất hữu cơ (đờm, máu, mủ...).
- Không gây ăn mòn với tất cả các loại dụng cụ.
3.1.2. Cơ chế tác dụng
Hoạt tính diệt khuẩn của Glutaraldehyde được thực hiện bởi việc kiềm hóa các nhóm: sulfhydral, hydroxyl, carboxyl và amino của vi sinh vật. Đây là nguyên nhân dẫn đến những thay đổi về cấu trúc AND, ARN và những thay đổi trong quá trình tổng hợp protein của vi sinh vật.
3.1.3. Hướng dẫn sử dụng
Dung dịch Glutaraldehyde ≥ 2% mang tính kiềm thường được sử dụng với mục đích khử khuẩn mức độ cao các dụng cụ kém chịu nhiệt như: ống nội soi, dụng cụ gây mê, dụng cụ đo dung tích phổi và các trang thiết bị khác sử dụng trong chẩn đoán, điều trị các bệnh đường hô hấp.
Dụng cụ sau khi ngâm trong dung dịch phải được tráng kỹ bằng nước cất vô khuẩn và làm khô rồi mới được mang ra sử dụng.
Nhân viên y tế có thể bị viêm da, kích ứng niêm mạc mũi, mắt... do phơi nhiễm với Glutaraldehyde khi dung dịch lưu giữ trong các chậu ngâm không được đậy kín hoặc do hệ thống thông khí tại khu vực xử lý dụng cụ không đủ tiêu chuẩn.
Trong những trường hợp như vậy, nồng độ Glutaraldehyde có thể đạt ở mức 0,05 ppm. Để làm giảm thiểu nguy cơ phơi nhiễm với dung dịch Glutaraldehyde trong quá trình sử dụng, các dung dịch cần được lưu giữ trong chậu có nắp đậy kín. Tốc độ trao đổi khí của hệ thống thông khí tại khu vực khử khuẩn dụng cụ phải đạt từ 7-15 luồng không khí trao đổi/giờ.
Nồng độ Glutaraldehyde giảm đi trong thời gian sử dụng, phải thường xuyên kiểm tra hiệu lực khử khuẩn của dung dịch.
3.2. Hydrogen peroxide
3.2.1. Đặc điểm chung
Hydrogen peroxide có hoạt tính diệt khuẩn tốt, diệt được vi khuẩn, vi rút, nấm và bào tử.
3.2.2. Cơ chế tác dụng
Hydrogen peroxide phá hủy gốc hydroxyl tự do, dẫn đến thay đổi cấu trúc màng lipid, DNA và các thành phần thiết yếu khác của tế bào vi sinh vật. Loại hóa chất này có khả năng ức chế khả năng sản xuất men catalase (men có tác dụng bảo vệ tế bào vi sinh vật chống lại tác động của Hydrogen peroxide bằng cách làm thoái hóa Hydrogen peroxide thành oxy và nước).
3.2.3. Hướng dẫn sử dụng
Dung dịch Hydrogen peroxide 6%-25% có tác dụng tiệt khuẩn. Những sản phẩm sử dụng phổ biến trên thị trường hiện nay là dung dịch chứa 7,5% Hydrogen peroxide và 0,85% Acid phosphoric (giúp dung dịch duy trì độ PH thấp. Dung dịch Hydrogen peroxide 5% bất hoạt 105 vi khuẩn lao đa kháng thuốc sau 10 phút, bất hoạt các vi rút bại liệt, viêm gan A sau 30 phút. Dung dịch Hydrogen peroxide 10% được so sánh về hiệu quả diệt khuẩn của dung dịch Glutaraldehyde 2% trong thời gian 20 phút.
Nồng độ Hydrogen peroxide giảm nhiều trong khi sử dụng, vì vậy cần phải thường xuyên kiểm tra hiệu lực khử khuẩn của dung dịch đã hoạt hóa.
3.3. Orthopthaladehyde
3.3.1. Đặc điểm chung
Orthopthaladehyde (OPA) là loại hợp chất chứa 0,55% 1.2 Benzendicarboxyl- aldehyde. OPA có khả năng diệt khuẩn tốt, đặc tính diệt vi khuẩn lao của OPA tốt hơn so với Glutaraldehyde.
3.3.2. Cơ chế tác dụng
Cơ chế tác dụng hiện nay vẫn chưa được xác định rõ.
3.3.3 Hướng dẫn sử dụng
Dung dịch OPA thường được sử dụng để khử khuẩn các dụng cụ nội soi. Hoạt tính diệt khuẩn của OPA ổn định trong phạm vi pH thay đổi từ 3-9. Không đòi hỏi phải hoạt hóa dung dịch trước khi sử dụng. OPA có tác dụng diệt khuẩn nhanh (ngâm ngập dụng cụ trong dung dịch sau 5 phút, vớt ra tráng lại bằng nước vô khuẩn và làm khô trước khi sử dụng).
3.4. Paracetic acid
3.4.1. Đặc điểm chung
Paracetic acid hay Acid peroxyacetic là hợp chất có tác dụng diệt khuẩn nhanh, phổ kháng khuẩn rộng. Các sản phẩm phân hủy sau sử dụng như Acid acetic, nước, oxy, Hydrogen peroxide không gây hại cho người sử dụng và không ảnh hưởng tới môi trường.
Paracetic acid có thể ăn mòn, làm mất độ bóng của dụng cụ kim loại. Dung dịch Paracetic acid khi pha loãng (1%) không có tính ổn định cao do xảy ra quá trình thủy phân trong dung dịch. Dung dịch 40% giảm 1-2% thành phần có hoạt tính trong 1 tháng.
3.4.2. Cơ chế tác dụng
Paracetic acid gây oxy hóa các liên kết sulphur trong phân tử protein của vi sinh vật làm thay đổi cấu trúc phân tử protein của chúng.
3.4.3. Hướng dẫn sử dụng
Dung dịch Paracetic acid nồng độ 0,2-0,35% có tác dụng tiệt khuẩn và bào tử rất tốt, thường được dùng để tiệt khuẩn các dụng cụ ngoại khoa, nội soi. Tính ổn định của dung dịch này rất thấp, thời hạn sử dụng không quá 24 giờ.
Bảng 2. Hiệu quả bất hoạt vi rút của các hoá chất khử khuẩn
|
Loại chất diệt khuẩn |
Nồng độ tối thiểu để bất hoạt 105 - 107 vi rút trong 10 phút |
|
|
Vi rút thuộc nhóm lipid (Adeno, Herpes, Influenza...) |
Virut thuộc nhóm Hydrophylic (EBOLA, Coxsackie, ECHO...) |
|
|
Sodium hypochlorite (Javel) |
200 ppm |
200 ppm |
|
Iodophor |
75 - 150 ppm |
150 ppm |
|
Formalin |
2% |
2-8% |
|
Glutaraldehyde |
0.02% |
1-2% |
|
Ethyl alcohol |
30-50% |
50 - 70% |
|
Isopropyl alcohol |
20-50% |
90% (Echo 6) 95% |
|
Phenol |
1-5% |
5% |
|
Phenyl phenol |
0.12% |
12% |
Bảng 3. Các hóa chất khử khuẩn có chứa Clo sử dụng trong phòng chống dịch bệnh COVID-19 tại các cơ sở khám bệnh, chữa bệnh.
|
Vị trí, thời điểm |
Nồng độ Clo hoạt tính |
Ghi chú |
|
Vệ sinh bề mặt khu vực thường (sàn, tường nhà, vật dụng) |
0,05% |
Nồng độ tối thiểu 0,05%, lau, xịt bề mặt không lau được |
|
Vệ sinh bề mặt khu vực cách li |
0,05% |
|
|
Bề mặt TTB, phương tiện trong phòng cách ly |
0,05% |
Lau, xịt (tùy theo vị trí) |
|
Xe, phương tiện vận chuyển người bệnh |
0,05% |
Nồng độ tối thiểu 0,05%, lau, xịt bề mặt không lau được |
|
Đổ tràn máu, dịch |
0,5% |
|
|
Chất thải (nước tiểu, phân, chất nôn, dịch hút...) |
1,0% |
Trộn theo tỉ lệ 1:1, đổ vào chất thải trong thời gian ít nhất 30 phút |
|
Bàn XN và TTB xét nghiệm |
0,5% |
Tham khảo hướng dẫn của nhà sản xuất thiết bị |
|
Xử lý thi hài |
0,5% |
Bọc kín thi hài bằng túi chuyên dụng lần thứ nhất, phun bên ngoài túi lần 1. Ngay sau khi chuyển ra khỏi phòng cách ly, tiếp tục bọc thi hài vào túi chuyên dụng lần 2, phun ngoài túi lần 2. |
|
Khử khuẩn dụng cụ, bề mặt bàn phẫu thuật, buồng phẫu thuật, phương tiện liên quan khâm liệm, phẫu thuật tử thi |
||
|
Dụng cụ ăn uống của NB |
0,05% |
Ngâm |
|
Đồ vải |
0,01%-0,05% |
Tùy thuộc vào tình trạng nhiễm bẩn máu, dịch và chất liệu vải |
Chú ý: Tùy theo mức độ sử dụng hóa chất, người sử dụng phải mang đầy đủ các phương tiện PHCN thích hợp để tránh các tác dụng phụ đối với cơ thể.
TÀI LIỆU THAM KHẢO
1. Hướng dẫn tạm thời giám sát và phòng, chống bệnh viêm phổi cấp do chủng Corona mới (nCoV), Quyết định số 181/QĐ-BYT ngày 21/01/2020 của Bộ trưởng Bộ Y tế.
2. Hướng dẫn tạm thời giám sát và phòng, chống bệnh viêm đường hô hấp cấp do chủng mới của vi rút Corona (nCoV), Quyết định số 343/QĐ-BYT ngày 07/02/2020.
3. Hướng dẫn Chẩn đoán và Điều trị bệnh viêm phổi cấp do nCoV, Quyết định số 125/QĐ-BYT ngày 16/01/2020 của Bộ trưởng Bộ Y tế.
4. Sổ tay hướng dẫn phòng ngừa lây nhiễm vi rút Corona gây Hội chứng viêm đường hô hấp cấp vùng Trung Đông (MERS-CoV), Cục Quản lý Khám, chữa bệnh, Bộ Y tế, 2015.
5. Quyết định số 3671/QĐ-BYT ngày 27/9/2012 của Bộ trưởng Bộ Y tế ban hành các hướng dẫn kiểm soát nhiễm khuẩn trong cơ sở khám bệnh, chữa bệnh.
6. Quyết định số 3916/QĐ-BYT ngày 28/8/2017 của Bộ trưởng Bộ Y tế ban hành các hướng dẫn kiểm soát nhiễm khuẩn trong cơ sở khám bệnh, chữa bệnh.
7. Novel Coronavirus (COVID-19) v3, World Health Organization, Last Update: 7 February 2020.
8. Laboratory biosafety guidance related to the novel coronavirus (2019- nCoV), World Health Organization, Interim guidance 12 February 2020.
9. Infection prevention and control of epidemic and pandemic-prone acute respiratory infections in health care, World Health Organization, 2014.
10. Infection prevention and control during health care when novel coronavi rút (nCoV) infection is suspected, Interim guidance, January 2020, WHO/2019- nCoV/IPC/v2020.1.
11. Advice on the use of masks the community, during home care and in health care settings in the context of the novel coronavi rút (2019-nCoV) outbreak, Interim guidance 29 January 2020, WHO/nCov/IPC_Masks/2020.1.
12. Transmission of Novel Coronavi rút (2019-nCoV)| CDC". www.cdc.gov. 27 January 2020. Archived from the original on 28 January 2020. Retrieved 29 January 2020.
13. "China confirms human-to-human transmission of new coronavirus". Canadian Broadcasting Corporation. 20 January 2020. Archived from the original on 20 January 2020. Retrieved 21 January 2020.
14. Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings (2007). Last update: July 2019.
15. Guideline for Disinfection and Sterilization in Healthcare Facilities, 2008, CDC, Update: May 2019.
Bạn chưa Đăng nhập thành viên.
Đây là tiện ích dành cho tài khoản thành viên. Vui lòng Đăng nhập để xem chi tiết. Nếu chưa có tài khoản, vui lòng Đăng ký tại đây!
Bạn chưa Đăng nhập thành viên.
Đây là tiện ích dành cho tài khoản thành viên. Vui lòng Đăng nhập để xem chi tiết. Nếu chưa có tài khoản, vui lòng Đăng ký tại đây!
